Contents
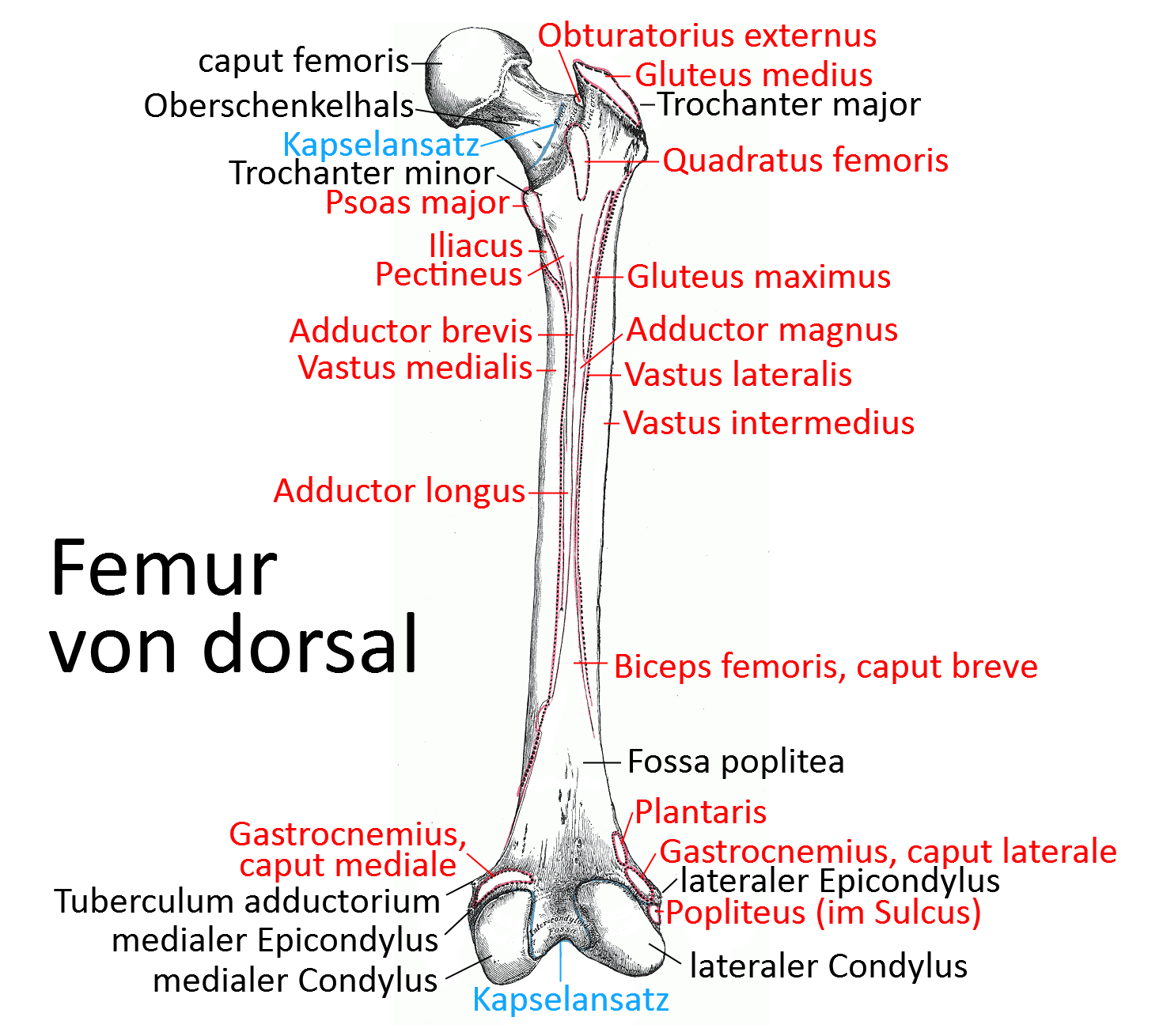
Image: Dorsal view of the femur (Linkmap)
Femur
Femur, consisting of a long shaft, the short neck, which form an angle(CCD angle) of 120° in adults, and the head, which articulates with the hip bone in the acetabulum.
The femur is the longest and strongest bone in the human body.
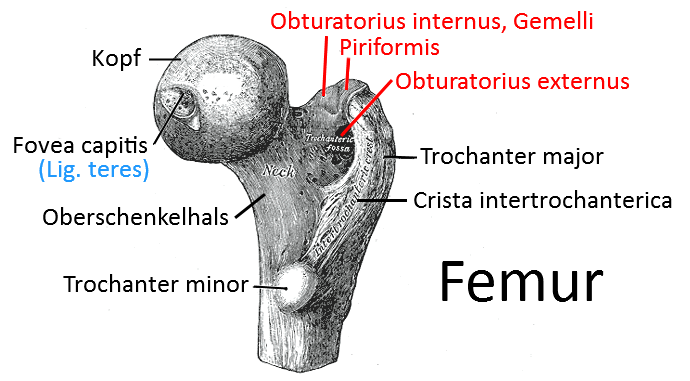
Head (caput ossis femoris, „femoral head“)
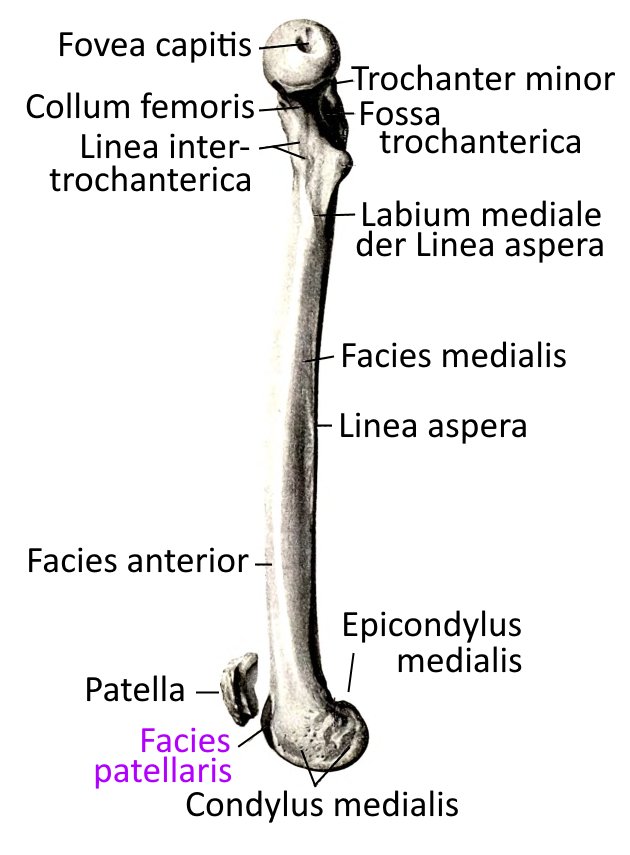
The femoral head is the part of the femur that articulates with the hip bone in the acetabulum . The articular surfaces are not exactly congruent, which allows better mobility. The fovea capitis femoris, into which a ligament(capitis femoris ligament) with an artery supplying the femoral head runs from the acetabulum, is located far in the middle of the spherical articular surface.
CCD angle
While the CCD angle is still around 137° in newborns and 130° during puberty, it decreases to the physiological 125°-120° by adulthood. It tends to be larger in young adults and smaller in later years. Deviations lead to incorrect loading of the lower extremity and all structures proximal to the femur and may require correction. If, for example, the arterial supply to the femoral head is impaired by an incorrect angle, this is a case of Perthes‘ disease requiring treatment. If the X-angle is too large, it is referred to as coxa valga, and if it is too small, it is referred to as coxa vara, as occurs with increased flexibility of the bone, for example in rickets.
Since the CCD angle is a statically and kinetically difficult construction and a predilection site for fractures, there is a tension belt from the side in the form of the iliotibial tract and the tensor fasciae latae tensioning it.
Other important proximal structures are the greater trochanter, which represents an extension of the lever arm for the muscles running over it, and the lesser trochanter as the insertion of the hip flexors.
Distally, there are the two femoral condyles, which together with the tibia form the knee joint, whereby their eminentia intercondylaris engages between the two femoral condyles and restricts displacement in the frontal vertebrae in addition to the collateral ligaments.
The meniscus also acts as a buffer between the cartilage-covered condyles of the femur and the tibia .
Trochanters
Trochanter major
Bony protrusion on the proximal lateral femoral shaftat the transition to the femoral neck, to which important muscles, including some of the dorsal hip muscles, attach:
The bony protrusion provides the attaching muscles with significantly better leverage.
Minor trochanter
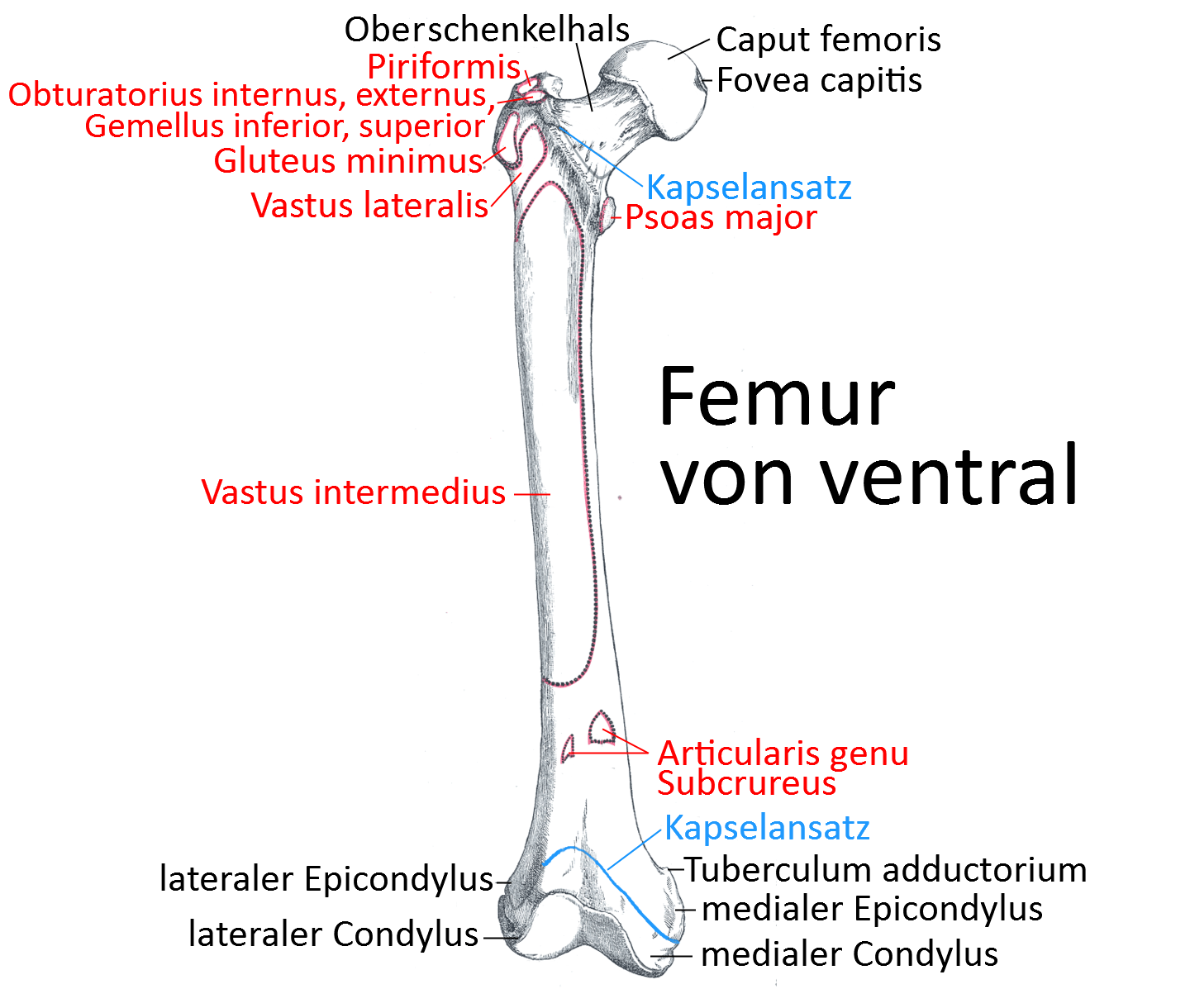
Bony protrusion on the proximal, slightly medial, more dorsal femoral shaft to which the iliopsoas, i.e. psoas major and iliacus, attaches.
Linea intertrochanterica
Ventrally, the two trochanters are separated from each other by the intertrochanteric line.
Linea intercondylaris
The intercondylar line is a small bony ridge that runs transversely between the two femoral condyles. It lies at the dorsal-cranial end of the intercondylar femoral fossa and, together with the lateral supracondylar linea and the medial supracondylar linea, forms an isosceles triangle known as the popliteal facies. The anterior cruciate ligament borders the linea intercondylaris with its anteromedial fiber bundle.
Crista intertrochanterica
The dorsal border between the torchanteres is the crista intertrochanterica.
Trochanteric fossa
The trochanteric fossa is the depression between the greater trochanter and the femoral neck (collum femoris). Several muscles attach to the trochanteric fossa:
Femoral neck
The short part of the femur that lies between the CCD angle and the head (femoral head). This part is particularly prone to fracture in osteoporotic bones.
The neck can have various geometric defects:
- Coxa vara – reduced CCD angle
- Coxa valga – enlarged CCD angle
- Coxa antetorta – greater antetorsion than normal
- coxa retrotorta – antetorsion of the femoral neck less than 0°
Shank
The shaft is the long, mainly vertical part of the femur that extends between the distal femoral condyles and the CCD angle. The shaft has a rough longitudinal line on its posterior side, the linea aspera, which is bordered by two caudally and cranially diverging ridges/lips (labium mediale and labium laterale). The labium laterale opens cranially into the gluteal tuberosity. The linea pectinea is another groin/lip parallel to the labium mediale that runs directly towards the lesser trochanter. Further distally, the two lips merge into the linea supracondylaris medialis and linea supracondylaris lateralis, which include the facies poplitea. All groins and lines are insertions of adductor muscles.
AT angle
The antetorsion angle (anteversion angle) is determined between the neck of the femur (collum femoris) and the dorsal plane tangential to the femoral condyles and parallel to the shaft. At birth, it is between 30° and 50° and gradually approaches a value between 10° and 15° with the end of growth. AT angles adapt much better to the target value/range as the child grows than in the case of the CCD angle. If the AT angle is greater than 30° at the end of growth, this is referred to as coxa antetorta; the exorotation of the hip joint is then restricted. An AT angle of less than 10° is coxa retrotorta. Both deviations impair the gait pattern.
Femoral condyles
The two bony prominences, the distalmost part of which articulates with the tibia in the knee joint by means of cartilage coverings. A distinction is made between the lateral condyle and the medial condyle. Both condyles open up a cavity, the cruciate ligament cavity (intercondylar notch). Ventrally, the condyles confluent to the articular surface with the patella facies patellaris(femoropatellar sliding bearing). Both condyles each form an epicondyle: (epicondylus medialis and epicondylus lateralis).
Condylus lateralis
The lateral condyle is the origin of the popliteus.
Condylus medialis
The medial condyle is the origin of the posterior cruciate ligament and the Wrisberg ligament.
Intercondylar fossa
The intercondylar fossa is the fossa that separates the two condyles. The dorsal border of the fossa is the intercondylar line.
Lateral epicondyle
The lateral collateral ligament and the lateral head of the gastrocnemius (origin) and the plantaris (origin) attach to the lateral epicondyle of the humerus. The lateral epicondyle has a lateral groove, the sulcus popliteus.
Medial epicondyle
The medial collateral ligament, the medial head of the gastrocnemius (origin) and the adductor magnus (insertion) are attached to the medial epicondyle of the humerus.
Joints
- Art. coxae(hip joint)
- Art. femorotibiais(knee joint, femorotibial joint)
- Art. femoropatellaris (femoropatellar sliding bearing, femoropatellar joint)
Pathology
- Fracture of the neck (femoral neck fracture)
- Fracture of the shaft (subtrochanteric fracture)
- Coxarthrosis(osteoarthritis of the femoral head)
- Coxitis(Arthritis des Hüftgeleks)
- Arthrose des Condylus lateralis und Condylus medialis
Images
Femur from ventral (image links to linkmap)
Femur from medial
Proximal end with femoral head (image links to linkmap)