yogabook / joints / pelvis / SI-Jiont
Contents
- 1 Image: Articular surface of the SI joint at the sacrum
- 2 Sacroiliac joint (sacroiliacjoint, articulatio sacroiliaca, articulatio iliosacralis, sacroiliac joint, SI joint)
- 3 Articulating bones
- 4 Ligaments
- 4.1 Lig. ileopectineum (Lig. cooperi)
- 4.2 iliolumbar ligament
- 4.3 Lig. inguinale (inguinal ligament, Vesalius ligament)
- 4.4 Lig. lacunare (Lig. gimbernati)
- 4.5 Lumbosacral ligament
- 4.6 Pubic ligament
- 4.7 Lig. pubicum superius
- 4.8 Lig. pubicum inferius (Lig. arcuatum pubis)
- 4.9 Lig. reflexum
- 4.10 Ligg. sacrococcygea
- 4.10.1 Lig. sacrococcygeum posterius profundum (dorsale profundum)
- 4.10.2 Lig. sacrococcygeum posterius superficiale (dorsal superficiale)Images:
- 4.10.3 Anterior sacrococcygeal ligament
- 4.10.4 Lig. sacrococcygeum interosseum (interosseum axiale)
- 4.10.5 Lateral sacrococcygeal ligament
- 4.10.6 Sacrococcygeal articular ligament (intraalticular)
- 4.11 Sacroiliac ligament
- 4.12 Sacrospinous ligament
- 4.13 Sacrotuberous ligament
- 5 Movements
- 6 Pathology
- 7 Tests
- 8 Images
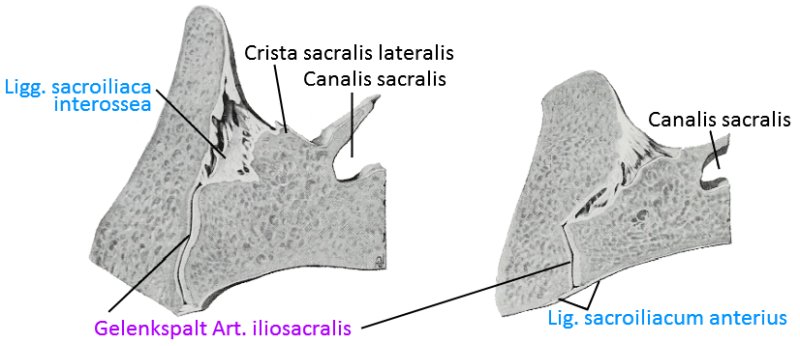
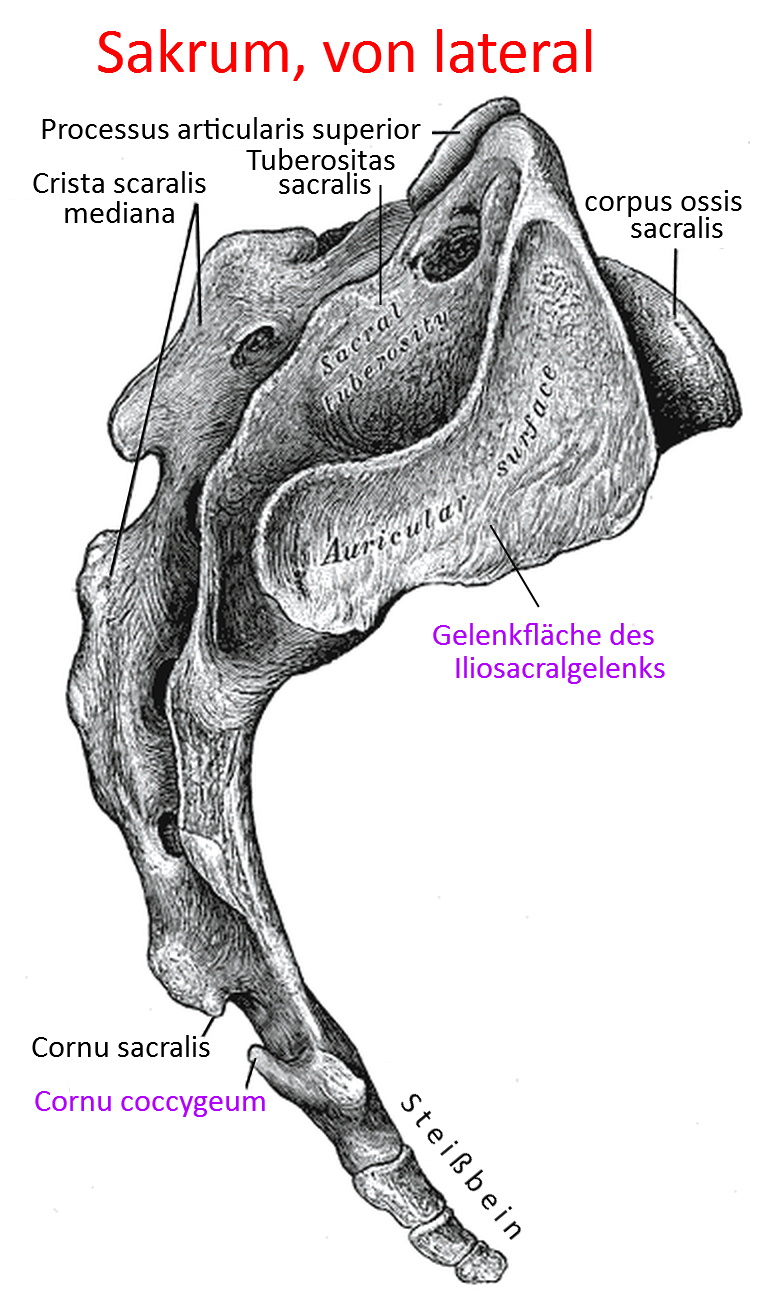
Image: Articular surface of the SI joint at the sacrum
Sacroiliac joint (sacroiliacjoint, articulatio sacroiliaca, articulatio iliosacralis, sacroiliac joint, SI joint)
The joint between the sacrum and iliac blades, i.e. the connection between the spine and pelvis. It is not constructed like the synovial joints of the extremities but is an amphiarthrosis with pronounced ligamentous protection and is therefore not designed for significant movements, but only allows a tilting movement („nutation“) of up to a maximum of 4°, in which the cranial base tilts ventrally-caudally around a transverse axis in relation to the caudal apex. The exact extent is still controversial and is given as 2 to 18 degrees, depending on the source. The SI joint is capable of further movements in a subordinate and very limited manner by opening up anteriorly or posteriorly. At around 18 cm², the SIJ has a very large joint surface. It is known that the mobility of the SIJ usually decreases with age. In males, grooves and elevations in the joint surfaces are more pronounced, so that in females stability depends more on muscles and ligaments, which means that deficits in these tissues are much more likely to lead to instability. Furthermore, the SI joint has a high degree of individual differences.
As the dorsal sacroiliac interosseous ligament and posterior sacroiliac ligament of the SI joint are very strong, the movement is mainly ventral and cranial. In particular, the apex moves dorsally and slightly cranially. The pelvic outlet is thus enlarged, the iliac tuberosities(ala ossis ischii) move closer together and the ischial tuberosities (ischial tuberosities) move apart.
The articular surface at the sacrum is covered by hyaline cartilage, while the fibrocartilage at the ilium is about half as thick. At a young age, the joint surfaces are flat; with increasing age, the joint surface in the sacrum deepens, while the surface on the ilium increases. Together with strong ligaments, this joint is therefore less prone to dislocation. Ventrally, the joint is stabilized primarily by the capsule; dorsally, the ligaments can be divided into short intrinsic and long extrinsic ligaments. The short interosseous ligaments, anterior sacroiliac ligament, posterior sacroiliac ligament and interosseous sacroiliac ligament are very strong and their tensile strength can exceed that of the bone. The extrinsic ligaments include the sacrotuberous ligament, the sacrospinous ligament and the iliolumbar ligament. The short intrinsic ligaments cover the joint approximately orthogonally to the joint space, while the long extrinsic ligaments run obliquely vertically. The ligaments of the SIJ loosen, particularly in the later stages of pregnancy under the influence of the hormone relaxin. In addition to securing the ligaments, the joint is held together by muscles: by the piriformis and by the gluteus maximus. The iliopsoas is also important as a powerful regional muscle.
One of the tasks of the SI joint is to cushion the impact of the large cranial partial body weight. The joint is shaped in such a way that it assumes its maximum congruence and stability (close packed position) at the end of the stance leg phase when walking, i.e. when the hip extensors push off. The SI joint tends to tilt in some people, which is often referred to as an SI joint blockage. In any case, the mobility of the SIJ decreases with age, and this is most pronounced in young women. Sometimes inflammation of the SIJ also occurs, especially in the context of the following underlying diseases:
- Ankylosing spondylitis
- Reiter’s disease (reactive arthritis)
- Behcet’s disease
- Psoriatic arthritis
- CED(ulcerative colitis and Crohn’s disease)
Osteoarthritis of the SI joint is also possible. Complaints in the SIJ can also be the result of acute or chronic incorrect loading, as well as regional fatigue fractures. Other possible causes include compression trauma, missteps and, of course, leg length discrepancies. The later stages of pregnancy are also often accompanied by SI joint complaints. A precise medical history with a thorough physical examination, in particular various tests, is a prerequisite for a reliable diagnosis. In the differential diagnosis, similarly localized disorders such as lumbago or lumbar disc hernias should also be considered. Pain is often caused less by the SI joint itself than by the regional fasciae and ligaments, which are heavily interspersed with nerves.
Statistically, every German suffers from lumbar pain at least once in their lifetime, around a quarter of which is caused by the SI joint.
If complaints of the SIJ are recurrent or difficult to stop, the SIJ can be surgically stiffened with an arthrodesis without any significant loss of function in the person’s movement options.
Articulating bones
Ligaments
- Lig. ileopectineum
- iliolumbar ligament
- Inguinal ligament
- Lacunar ligament
- Lumbosacral ligament
- Lig. pubicum
- Lig. pubicum inferius
- Lig. pubicum superius
- Lig. reflexum
- Ligg. sarcococcygea
- Lig. sacrococcygeum anterius
- Lig. sacrococcygeum articulare
- Lig. sacrococcygeum interosseum
- Lig. sacrococcygeum laterale
- Ligg. sarcococcygea posterius profundum
- Ligg. sarcococcygea posterius superficiale
- Ligg. sacroiliaca anteriora
- Ligg. sacroiliaca posteriora
- Ligg. sacroiliaca interossea
- Lig. sacroiliacum anterius
- Lig. sacroiliacum posterius brevis
- Lig. sacroiliacum posterius longus
- Lig. sacrospinale
- Sacrotuberous ligament
The tapes in detail
Lig. ileopectineum (Lig. cooperi)
The ileopectineal ligament is an extension of the lacunar ligament, which runs along the pecten ossis pubis of the ramus superior ossis pubis.
Images:
Linkmap: Trunk, lateral, very deep
Linkmap: Trunk, ventral view
Linkmap: Trunk ventral, semi-profound
Linkmap: Trunk, abdomen and chest
Linkmap: Torso, abdominal wall, from the inside
Torso, abdominal wall from diagonally inside
iliolumbar ligament
The iliolumbar ligament runs from medial-cranial to lateral-caudal from the costal process of LWK 4 and LWK 5 to the iliac crest and the anterior sacroiliac ligaments. It thus limits the lateral movement of the cranial pelvis.
Images:
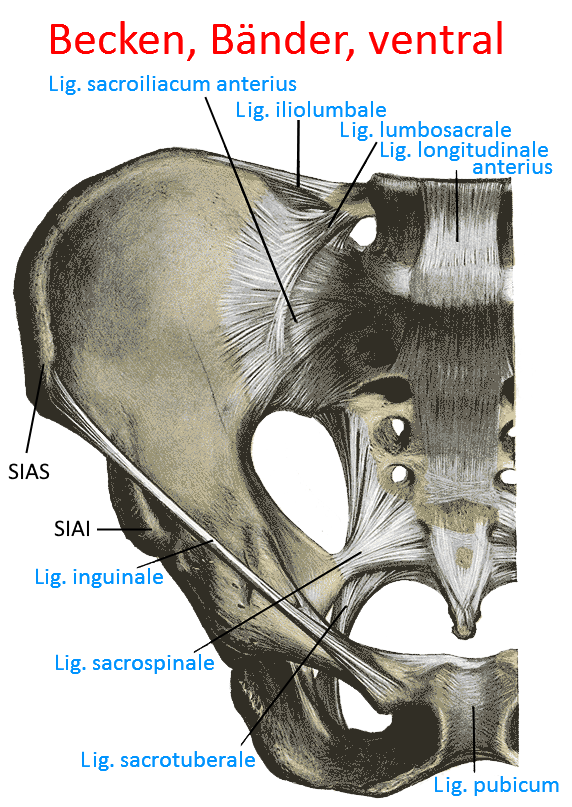
Linkmap: Pelvis, ventral ligaments
Linkmap: Trunk, posterior abdominal wall from ventral
Lig. inguinale (inguinal ligament, Vesalius ligament)
The inguinal ligament is a strong band from the anterior superior iliac spine to the pubic tubercle of the pubic bone. It arises from the aponeuroses of(obliquus externus abdominis, obliquus internus abdominis and transversus abdominis) and transverse fibrous cords of the iliac fascia. It represents the anterior and inferior wall of the inguinal canal. The anterior fibrous cords of the facia lata arise from anterior cords of the inguinal ligament.
Images:
Linkmap: Pelvis, ligaments, ventral
Linkmap: Acetabulum in context
Linkmap: Trunk, lateral, superficial
Linkmap: Trunk, lateral, profound
Linkmap: Trunk, lateral, very profound
Linkmap: Trunk, medium-profound
Linkmap: Trunk, ventral
Linkmap: Trunk, abdomen and chest
Linkmap: Trunk, posterior abdominal wall from ventral view
Linkmap: Pelvis, ligaments from ventral view
Linkmap: Inguinal ligament
Lig. lacunare (Lig. gimbernati)
The lacunar ligament is a short ventral ligament in the inguinal region that attaches cranially to the inguinal ligament and caudally to the pubic crest (pecten ossis pubis). It is delta-shaped and narrows medially. It can be understood as arising from the aponeurosis of the obliquus externus abdominis.
Images:
Linkmap: Trunk, lateral, profound
Linkmap: Trunk, abdominal wall, from oblique inside
Linkmap: Pelvis, ligaments from ventral
Linkmap: Inguinal ligament
Lumbosacral ligament
The lumbosacral ligament begins at the level of Th8, extends caudally and runs
as a filum terminale to the posterior surface of the Os coccygis. On the way, it runs broadly to the lumbar spine and the intervertebral discs.
Images:
Linkmap: Pelvis, ligaments, ventral
Pubic ligament
The pubic ligament consists of the superior pubic ligament and the inferior pubic ligament, between which lies the interpubic disc into which both ligaments radiate.
Images:
Linkmap: Pelvis, ligaments, ventral
Lig. pubicum superius
The inferior pubic ligament is the upper ligament of the pubicsymphysis that radiates into the interpubic disc.
Images: (still without)
Lig. pubicum inferius (Lig. arcuatum pubis)
The inferior pubic ligament is the lower ligament of the pubicsymphysis that radiates into the interpubic disc.
Images: (still without)
Lig. reflexum
The reflex ligament runs from the pubic tubercle and lacunar ligament craniomedially to the rectus sheath (anterior leaflet) and thus forms the medial floor of the inguinal canal and the dorsal border of the superficial inguinal annulus. The ligament arises from deep tendon fibers of the obliquus externus abdominis and can be seen as a separation of the inguinal ligament.
Images:
Linkmap: Inguinal ligament
Ligg. sacrococcygea
Lig. sacrococcygeum posterius profundum (dorsale profundum)
Das Lig. sacrococcygeum posterius profundus ist die Fortsetzung des Lig. longitudinale posterius vom Sacrum zum Steißbein.
Bilder:
Lig. sacrococcygeum posterius superficiale (dorsal superficiale)
Images:
The posterior superficial sacrococcygeal ligament is the continuation of the supraspinous ligament from the sacrum to the coccyx. It runs from the sacral hiatus to S2.
Images:
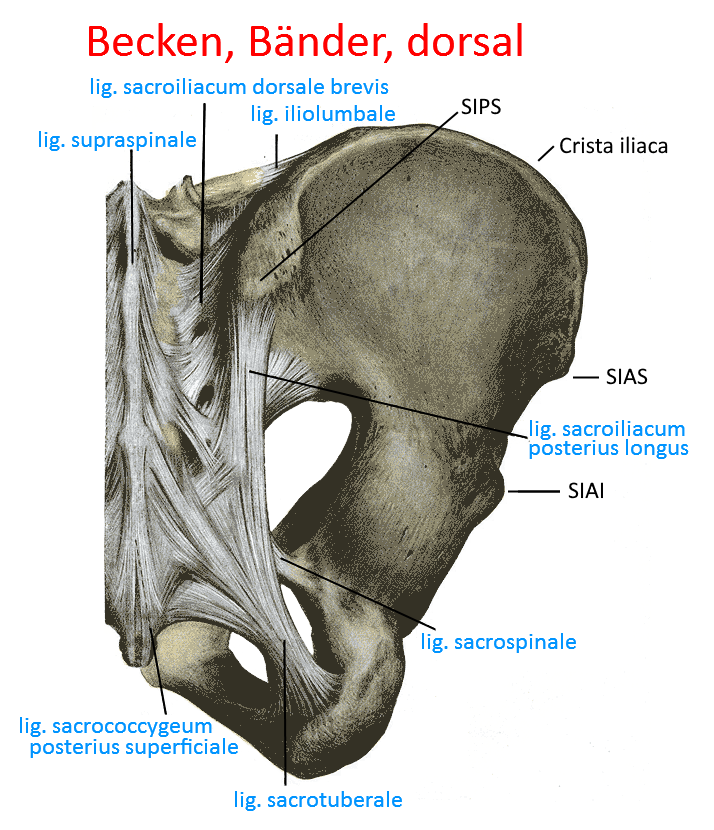
Linkmap: Pelvis, ligaments, dorsal
Linkmap: Trunk, dorsal, profound
Anterior sacrococcygeal ligament
The anterior sacrococcygeal ligament connects the ventral sides of the sacrum (Os sacrum) and coccyx (Os coccygis).
Images: (still without)
Lig. sacrococcygeum interosseum (interosseum axiale)
The sacrococcygeal interosseous ligament connects the tuberosities of the sacrum with the ilium.
Images: (still without)
Lateral sacrococcygeal ligament
The lateral sacrococcygeal ligament runs from the lower lateral edge of the sacrum to the transverse process of the coccyx.
Images:
Linkmap: Torso, dorsal, profound
Sacrococcygeal articular ligament (intraalticular)
The sacrococcygeal articular ligament connects the cornu of the sacrum with the cornu of the coccyx.
Images:
Linkmap: Trunk, dorsal, profound
Sacroiliac ligament
Anterior sacroiliac ligament
The anterior sacroiliac ligaments run ventrally of the SI joint from the sacrum (especially from its two cranial root canals) to the hip bone. They delimit the greater sciatic foramen cranially.
Images:
Linkmap: Trunk, posterior abdominal wall, ventral
Anterior sacroiliac ligament
The anterior sacroiliac ligament is a collection of coarse, fibrous ligaments extending from the ventral side of S1 and S2 to the iliac bone.
Images:
Linkmap: SI-joint, sections
Linkmap: Pelvis, ligaments, ventral
Posterior sacroiliac ligament
The posterior sacroiliac ligament is a collection of coarse, fiber-rich ligaments that extend from the iliac tuberosity to the sacrum and serve as the origin of the multifidi.
Images: (still without)
Ligg. sacroiliaca posteriora (dorsalia)
The anterior sacroiliac ligaments(longus and brevis) run dorsally of the SI joint from the sacrum (especially from its cranial two WK) to the hip bone. They delimit the cranial foramen ischiadicum majus.
Images: (still without)
Lig. sacroiliacum posterius (dorsal) brevis
The posterior sacroiliac ligament runs from the dorsal surface of the sacrum (crista sacralis intermedia and lateralis) to the posterior inner surface(ventral) of the hip bone (iliac tuberosity).
Images: Linkmap: Pelvis, ligaments, dorsal
Lig. sacroiliacum posterius (dorsale) longus
The dorsal sacroliac ligament longus extends caudally in front of the dorsocranial edge of the iliac crest (SPIS, posterior superior iliac spine) and radiates into the sacrotuberous ligament on the one hand; on the other hand, fiber bundles extend medially to the lateral sacral crest of the caudal posterior sacrum.
Images: Linkmap: Pelvis, ligaments, dorsal
Ligg. sacroiliaca interossea
The posterior sacroiliac ligaments are strong ligaments between the sacral tuberosity and the iliac tuberosity. Both bone roughenings lie craniodorsal to the auricular facies. The interosseous sacroiliac ligaments lie deeper than the posterior sacroiliac ligaments.
Images:
Linkmap: SI-joint, sections
Sacrospinous ligament
The sacrospinous ligament runs from the sacrum and coccyx to the ischial spine of the ischium. This ligament lies between the foramen ischioadicum majus(cranial) and foramen ischiadicum minus(caudal).
Images:
Linkmap: Hip joint
Linkmap: Pelvis, ligaments, dorsal
Linkmap: Pelvis, ligaments, ventral
Linkmap: Trunk, lateral, superficial
Linkmap: Trunk, lateral, very deep
Linkmap: Trunk, medium-profound
Linkmap: Trunk, dorsal, profound
Linkmap: Torso, abdominal wall from oblique inside
Sacrotuberous ligament
The sacrospinous ligament runs from the sacrum and coccyx to the ischial tuberosity of the ischium. It forms the lower boundary of the lesser sciatic foramen and, together with the sacrospinous l igament, prevents the sacrum from tilting dorsally.
Images:
Linkmap: Hip joint
Linkmap: Pelvis, ligaments, dorsal
Linkmap: Pelvis, ligaments, ventral
Linkmap: Acetabulum in context
Linkmap: Trunk, lateral, superficial
Linkmap: Trunk, lateral, very deep
Linkmap: Trunk, medium-profound
Linkmap: Trunk, dorsal, profound
Linkmap: Trunk, dorsal
Movements
Nutation (tilting movement of max. 4°), contranutation, a tilting movement in the saggital plane.
Pathology
Tests
Tests of the SI-joint
General tests
- Mennell-Test (distinction hip joint – sarcoiliac joint)
Instability
- Spine_test
- Maigne Test
- Stauchungstest
- Standing Bent Over Test (Vorlauf-Phänomen)
- Laslett-Cluster
- van der Wurff Cluster
- Gänslen sign
- Shimpi Prone SI Joint Test
- Gilet test
- Yeoman test
Tests of the movement directions
Tests of the spanning muscles
Images
Ligaments from ventral (image links to linkmap)
Ligaments from dorsal (image links to linkmap)
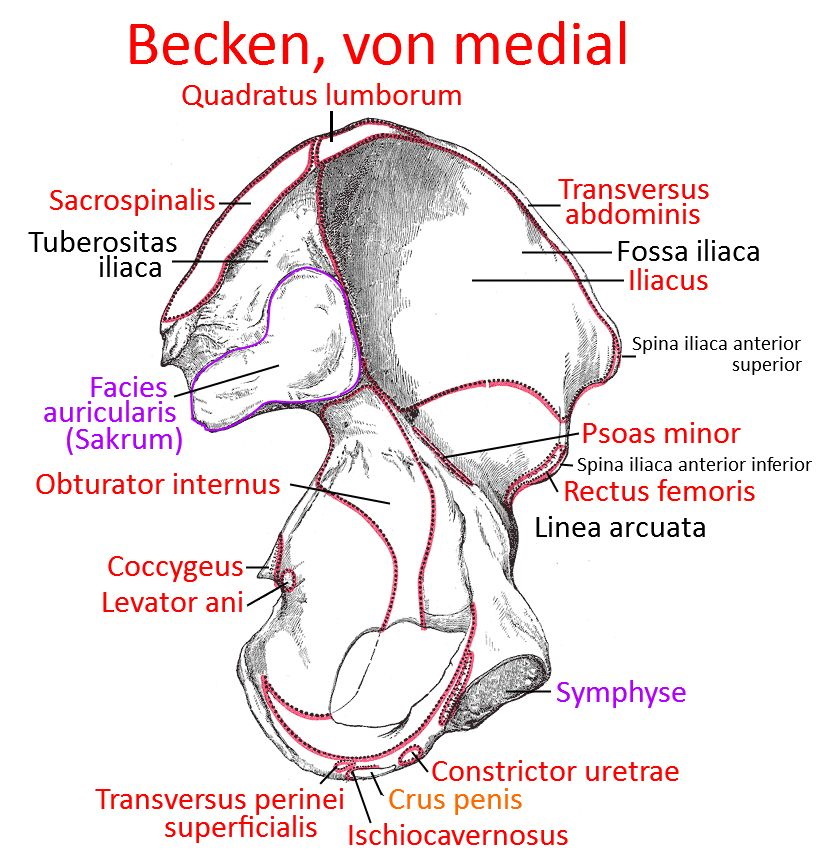
Pelvis from medial (image links to linkmap)
Parallel sections through the linea terminalis, cranial and caudal through the SI joint (image links to linkmap)