yogabook / movement physiology / nervous system
Contents
- 1 Sympathetic
- 2 Sympathetic nervous system
- 3 Parasympathetic tone
- 4 Parasympathetic nervous system
- 5 Brachial plexus
- 6 Cauda equina
- 7 cranial nerves
- 8 Hirnnerven
- 9 Dermatome
- 10 Distinctive muscles
- 11 Functional pain
- 12 Golgi tendon organ
- 13 N. vagus, vagus nerve
- 14 N. vagus
- 15 Proprioception
- 16 Proprioceptors
- 17 Pseudoradicular pain
- 18 Radicular pain
- 19 Sciatic nerve
- 20 Spinal canal
- 21 Spinal cord
- 22 Spinal nerve
- 23 Structural pain
- 24 Vagus nerve (N. vagus)
- 25 Vagotone
Sympathetic
State of increased excitation of the sympathetic nervous system.
Sympathetic nervous system
The sympathetic nervous system is the part of the autonomic nervous system that controls the increase in performance and mobilization of energy reserves. These effects are referred to as ergotropic. It is largely antagonistic to the parasympathetic nervous system. On the heart, the sympathetic nervous system is positively chronotropic, positively dromotropic (accelerating stimulus conduction), positively inotropic (increasing contraction force), positively bathmotropic (lowering the stimulus threshold), positively lutitropic (promoting relaxation) and thus increases cardiac output in every possible way. In the blood vessels it has a vasoconstrictive effect, dilates the bronchi and inhibits mucus production and liquefies mucus, in the gastrointestinal tract it reduces gland secretion and peristalsis, in the genitourinary tract it tightens the bladder sphincter and weakens the detrusor vesicae muscle, in the eye it causes mydriasis (dilation of the pupil) and generally leads to increased sweat secretion. Increased excitation of the sympathetic nervous system is referred to as sympathetic tone and has a weakening effect on HRV.
Parasympathetic tone
State of increased excitation of the parasympathetic nervous system.
Parasympathetic nervous system
The parasympathetic nervous system is the part of the autonomic nervous system that is responsible for regeneration and building up energy reserves and is therefore largely the opposite of the ergotropic sympathetic nervous system, which controls the increase in performance and mobilization of energy reserves. These effects of the sympathetic nervous system are referred to as ergotropic. It is therefore largely antagonistic to the parasympathetic nervous system. The nerve fibers of the parasympathetic nervous system include some of the cranial nerves III (oculomotor nerve), VII (facial nerve), IX (glossopharyngeal nerve) and especially X (vagus nerve). The trigeminal nerve also carries sections of parasympathetic fibers, but these originate from the facial nerve. The parasympathetic nervous system has a negative chronotropic and negative dromotropic effect on the heart (promoting excitation conduction), has a vasodilatory effect on the vessels in the genital area, is constrictive and promotes mucus secretion in the bronchi, increases secretion and peristalsis in the digestive tract, promotes micturition in the genitourinary system, promotes contraction of the uterus, promotes miosis (pupil constriction) and accommodation and promotes saliva production. Increased excitation of the parasympathetic nervous system is referred to as parasympathetic tone or usually as vagal tone and has an HRV-enhancing effect.
Brachial plexus
As part of the PNS, the brachial plexus is a nerve plexus consisting of the ventral branches of the spinal nerves of the last four cervical spine segments and the first thoracic spine segment (C5-Th1) as well as smaller bundles of C4 and Th2. Compression of the brachial plexus can lead to thoracic outlet syndrome.
Cauda equina
from Latin: caeuda equina, horse’s tail, refers to the nerve roots of the spinal nerves that continue caudally towards the sacrum after the end (conus medullaris, approximately level L1) of the spinal cord and leave the spinal column through their corresponding intervertebral foramina.
cranial nerves
Hirnnerven
Die Hirnnerven treten paarig aus dem Schädel aus und leiten Signale von oder zum Gehirn.
I N. olfactorius leitet Signale von der Nase zum Gehirn und ermöglicht das Riechen
II N. opticus leitet Signale vom Auge zum Gehirn und ermöglicht das Sehen
III N. oculomotorius steuert Augenbewegungen, den Lidheber und die Iris (Regenbogenhaut)
IV N. trochlearis steuert den schrägen oberen Augenmuskel
V N. trigeminus unterteilt sich in ophtalmicus, maxillaris und mandibularis, leitet Signale aus dem Gesicht ans Hirn und steuert die Kaumuskulatur
VI N. abducens steuert den lateralen Augenmuskel
VII N. fascialis steuert die mimische Muskulatur und den M. stapedius (Mittelohr), leitet geschmackssensorische Reize der vorderen zwei Drittel der Zunge zum Gehirn, innerviert alls Kopfdrüsen mit Ausnahme der Parotis
VIII N. vestibulococclearis leitet Signale der Hörschnecken und des Gleichgewichtsorgans ans Gehirn
IX N. glossopharyngeus innerviert die Rachenmuskeln und steuert das Schlucken, leitet sensorische Reize des hinteren Drittelns der Zunge zum Hirn
X N. vagus wichtigster Nerv des Parasympathikus, steuert viele innere Organe mit, auch das Herz
XI N. accessorius steuert den Trapezius und den Sternocleidomastoideus
XII N. hypoglossus steuert die Bewegungen der Zunge
Zuweilen wird der N. terminalis als Nullter Nirnnerv (vermutlich Wahrnehmung von Pheromonen) bezeichnet und der zum N. fascialis gehörige N. intermedius als 13. Hirnnerv.
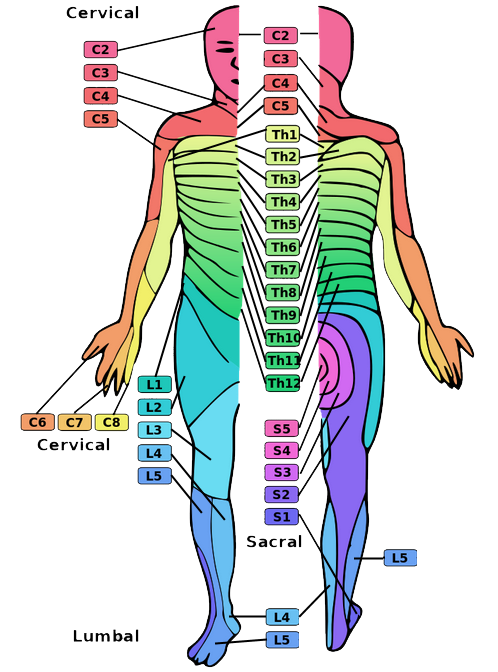
Dermatome
A dermatome is the area of skin supplied by a spinal nerve.
See this illustration.
{kind=link}
Distinctive muscles
Identifier muscles are muscles that are tested as a proxy for a myotoma and a spinal nerve in clinical testing, for example if there is suspected damage to a segment of the spine.
- C4: diaphragm
- C5: deltoid, infraspinatus, supraspinatus, rhomboids
- C6: biceps, brachioradialis
- C7: triceps, pronator teres, extensor carpi radialis, flexor carpi radialis, pectoralis major
- C8: interossei, abductor pollicis brevis, abductor digiti minimi, flexor carpi ulnaris, flexor pollicis brevis
- Th10-Th12: abdominal muscles
- L1: cremaster
- L3: quadriceps, iliopsoas, adductor longus, adductor brevis, adductor magnus
- L4: quadriceps femoris: vastus lateralis
- L5: fibularis longus, extensor hallucis longus, tibialis anterior, tibialis posterior, gluteus medius
- S1: triceps surae, gluteus maximus
- S2: flexor digitorum brevis
- S3/S4: bulbospongiosus
- S4/S5: sphincter ani externus
Some of the characteristic muscles can be tested with very simple tests:
- Quadriceps: squat
- Triceps surae: toe stand
- Tibialis anterior: ball of foot stand
Functional pain
Functional pain is not a clearly defined term. As a rule, it is understood to mean pain without a detectable non-clinical correlate, which could consist of evidence of inflammation, a fracture, bursitis, a torn muscle fiber, osteoarthritis or other manifest, detectable disorders. Functional pain is often understood to include pain caused by disorders that are detectable by appropriate means but are only slightly noticeable, such as the degenerative symptoms of insertional tendinopathy (enthesiopathy). Classic functional pain includes muscle tension, but also alterations in the capsular or ligamentous tension of the joints. The conceptual counterpart to functional pain is structural pain.
Golgi tendon organ
Nerve plexus at the transition from the contractile muscle belly to the tendon, which reports the state of tension (generally corresponds to the
tendon strength of the muscle) to the CNS. In the sense of autogenous inhibition, the motor neuron of this muscle is inhibited, i.e. the stimulus for further contraction is dampened, but at the same time the antagonist is stimulated via excitatory switching neurons (interneurons). Autogenic inhibition serves to regulate muscle tension and protect against overstraining. The Golgi tendon organ is one of the proprioceptors.
N. vagus, vagus nerve
The vagus nerve an antagonist to the sympathetic nervous system and the most important part of the parasympathetic nervous system. It is the 10th cranial nerve and is the only one that moves from the head into the trunk, hence its name translated as „wandering“. Among other things, it controls digestion and calms the heart, see the effects of the parasympathetic nervous system and heart rate variability (HRV).
N. vagus
The vagus nerve an antagonist to the sympathetic nervous system and the most important part of the parasympathetic nervous system. It is the 10th cranial nerve and is the only one that moves from the head into the trunk, hence its name translated as „wandering“. Among other things, it controls digestion and calms the heart, see the effects of the parasympathetic nervous system and heart rate variability (HRV).
Proprioception
Self-perception of the body independent of external sensors, i.e. the 5 senses. Proprioception makes it possible to perceive the position of the body in space and the position of the individual body parts in relation to each other, as well as the tension of the muscles and the force exerted. A distinction is made between
- Joint position sense: Sense of the geometric position of the body and joints
- Sense of movement (kinethesia): continuous sensation of changes in the position of the body or body parts
- Sense of force and resistance: Sensation of tension and pressure.
The sensors responsible for this are called proprioceptors:
- Muscle spindle: fibers arranged in the muscle parallel to the muscle fibers, which record the proportional behavior, i.e. the absolute length of a muscle with static core fibers and the differential behavior, i.e. the change in length, with dynamic core fibers.
- Tendon spindle (also: Golgi organ, Golgi tendon receptor): slow-adapting tension sensors located in the transition area between muscle and tendon fibers, basis of proprioceptive reflexes
- Sensitive receptors in joint capsule, ligaments, periosteum
In contrast to proprioception, visceroception enables the perception of internal organs. Both together are also referred to as interoception. Various proprioceptors are present for this purpose.
A distinction can be made between conscious proprioception, which is evaluated during conscious and targeted movements such as balancing or yoga poses, and unconscious proprioception, which is sufficient for mechanical movements such as walking or climbing stairs.
Proprioceptors
The receptors that enable proprioception are:
- Muscle spindle: fibers arranged in the muscle parallel to the muscle fibers, which record the proportional behavior, i.e. the absolute length of a muscle with static core fibers and the differential behavior, i.e. the change in length, with dynamic core fibers.
- Tendon spindle (also: Golgi organ, Golgi tendon receptor): slow-adapting tension sensors located in the transition area between muscle and tendon fibers, basis of proprioceptive reflexes
- Sensitive receptors in joint capsule, ligaments, periosteum
Pseudoradicular pain
Non-specific, localized pain with radiation („referred pain“) in the direction of an extremity similar to a radicular pain symptom, but without its efferent or afferent neurological deficits (in the area of innervation or sensitivity), as the spinal nerve itself is not impaired in its function. Pseudoradicular pain occurs, for example, as a result of facet syndrome, muscular or joint disorders and SI joint blockages.
Radicular pain
Pain caused by irritation (e.g. pressure) of a nerve root, as occurs in nerve root compression syndrome (radiculopathy). This is usually caused by intervertebral disc damage, osteophytes or inflammation. The pain typically projects into the dermatome of a nerve root. Radicular pain requires clarification and often also treatment. The compression of nerves can lead to their atrophy, but also to atrophy of the supplied musculature. The term neuroradicular is also used synonymously. See the difference to pseudoradicular here.
Sciatic nerve
The common fibular nerve and tibial nerve, which are wrapped together in connective tissue, are referred to as the „sciatic nerve“. Both emerge independently from the lumbosacral plexus, but pass through the intrapiriform foramen in a common sheath. The sciatic nerve supplies the lower extremity, with all flexors (exception: biceps femoris caput breve) of the knee joint and talocrural joint being supplied by the tibial nerve and the extensors and pronators of the ankle joints being supplied by the common fibular nerve. If the nerve is irritated or compressed in its course, whether it is the underlying spinal nerves or the sciatic nerve in its course in the dorsal hip area, disorders such as sciatica or lumbalgia or ischialgiform or lumbalgiform pain occur. However, these can also be caused simply by compression by a muscle, as in piriformis syndrome/deepgluteal syndrome DGS. Similar disorders also occur if the relevant nerves are compressed while still in the spinal canal, such as in spondylolisthesis or spinal canal stenosis, so that these disorders must be distinguished in a differential diagnosis. In some cases, this is already possible with the help of anamnesis and provocation tests, otherwise imaging such as MRI must be used. Irritation of the sciatic nerve can also be triggered by the effects of cold or pressure (sometimes associated with DGS ). Similar pain occurs in facet syndrome, but it is pseudoradicular and not radicular and does not cause muscular or sensitive deficits.
Spinal canal
The spinal canal in which the spinal cord runs and from which the spinal nerves emerge through the vertebral foramina.
Spinal cord
(lat. medulla spinalis or medulla dorsalis) part of the central nervous system that runs in the spinal canal. The spinal cord ends caudally as the conus medullaris (medullary cone) in the L1 / L2 area, where the nerves continue to run individually as the cauda equina. The existence of a spinal cord is common to all vertebrates. It is enveloped by meninges (from outside to inside: dura mater, arachnoid, pia mater), which in turn are surrounded by cerebrospinal fluid. Cranially, the spinal cord emerges from the medulla oblongata above the foramen magnum. The spinal cord contains the gray and white matter. For a more detailed description, see Wikipedia, for example.
Spinal nerve
The spinal nerves are the nerves that emerge from the spinal cord in pairs (right/left). From their exit from the spinal cord, they are part of the PNS. The spinal nerv es unite the anterior and posterior afferent and efferent nerve roots: afferents with sensory information enter through the posterior nerve root (radix posterior), efferents with motor nerve fibers and partly also fibers of the vagus nerve exit through the anterior nerve root. Pressure on a nerve root or the spinal nerve containing it can lead to a nerve compression syndrome. The nerve roots already join in the spinal canal.
Structural pain
Structural pain, like its conceptual opposite, functional pain, is not sufficiently clearly defined. Structural pain is pain caused by a (often: not too complex) detectable disorder such as inflammation, a fracture, a bursitis, a torn muscle fiber or osteoarthritis/arthrosis.
Vagus nerve (N. vagus)
The vagus nerve is the antagonist of the sympathetic nervous system and the most important part of the parasympathetic nervous system. It is the 10th cranial nerve and is the only one that moves from the head into the trunk, hence its name „wandering“. Among other things, it controls digestion and calms the heart, see the effects of the parasympathetic nervous system and heart rate variability (HRV).
Vagotone
State of increased excitation of the vagus nerve.