Contents
virasana
„hero“

Detailfotos
first: pull your knees forward | then: turn out the calves | afterwards: pull your bottom backwards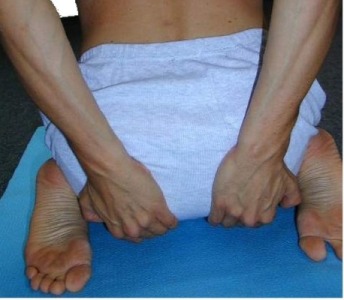 |
Feedback: We would love to hear what you think about this description, give us feedback at:
postmeister@yogabook.org
last update: 30.12.2018
Name: virasana
Trivial name: Hero
Level: A
- Classification
- Contraindication
- Effects
- Preparation
- Follow-up
- derived asanas
- similar asanas
- Diagnostics
- Instructions
- Details
- Variants
Classification
classical: sitting posture
psychomental:
physiological: quadriceps stretching(monoarticular parts)
Contraindication
Effects
- (811) Stretching the quadriceps
- (841) Stretching the foot lifts
- (871) Stretching the pronators of the ankle (limited)
Preparation
Virasana is the cardinal pose for stretching the monoarticular parts of the quadriceps, i.e. to be able to bend the knee joint completely; there are generally no preparatory exercises, but synergistic exercises are particularly important:
Follow-up
Sometimes after virasana there is a feeling of not being able to stretch the knee joints properly, especially if the quadriceps and hamstrings are not yet very flexible. Then try to slowly stretch them again in:
derived asanas:
similar asanas:
- supta virasana
- Quadriceps stretch 1
- Quadriceps stretch 2
- krouncasana
- supta krouncasana
- ardha supta krouncasana
Diagnostics (No.)
(650) Kyphosis and lordosis of the spine:
The deviations from the physiological double-S shape of the human spine are clearly visible in this posture. There should be a certain degree of lordosis (convex spine from the front) in the lumbar and cervical spine and a certain degree of kyphosis (convex spine from the back) in the thoracic spine. See the FAQ. If the short hip extensors are very inflexible, the pelvis may tilt backwards so that the physiological lordosis of the lumbar spine is lost and the kyphosis of the thoracic spine may also be more pronounced.
(611) Pelvic obliquity/unequal shoulder height/scoliosis of the spine:
The lateral deviations of the spine from the median plane known as scolioses are also quite visible in this posture. See the FAQ.
The main cause of the inability to bend the knee joint to the extent that the ischial tuberosities transfer the majority of the body’s gravitational force to the ground is the restricted flexibility of the monoarticular quadriceps parts.
In this position, knee problems associated with wide flexion become very apparent. These can be, for example: traumatic or degenerative meniscus damage, arthrosis, arthritis, subluxations, ligament damage, plica syndrome and others, see the FAQ.
Variants:
Instructions
- Sit on your lower legs. Bring your knees together.
- Raise the pelvis and bring the feet so far apart that the pelvis is exactly between the feet. Straighten the ankles.
- Press the backs of your feet to the floor and pull one knee forward at a time by reaching under the knee, pulling it forward and putting it down again. Your lower legs and feet should now be in a line that converges towards your knees.
- Grasp your calves and turn them out. Then slowly lower your pelvis until you are sitting firmly on the ischial tuberosities. The distance between your pelvis and ankle or heel should be zero.
- Use your hands to pull your buttocks back and stretch your torso upwards with your head in line with your torso.
- Turn your arms out and place the palms of your hands on the soles of your feet pointing upwards.
Details
- There should be no air between the pelvis and foot, and in particular it should not be possible to insert a hand between them. Any distance between the pelvis and foot can have a detrimental effect on the knee joint.
- The ankle joint must extend as straight as possible from the lower leg, which means: 180° angle in the ankle joint or the most precise plantar flexion possible. Any inward pivoting of the foot (as well as the distance between the pelvis and foot, see above) can lead to pressure in the outer knee and possibly destabilize the outer area of the ankle. In particular, never sit in virasana with your feet turned outwards, as is sometimes possible with mobile people, as this is not good for the knee joint. As there is only limited end rotation available in the hip joint, the rest of the rotation remains „stuck on the knee joint „, in which such a degree of rotation is unphysiological.
- The often occurring tendency to cramp in the sole of the foot is a phenomenon that depends on several factors, one of which is almost always an insufficiently stretched ankle. Reaching under the knee to lift it up and put it down again pulled forwards is a good way of preventing cramp and can be done several times. This measure causes the back of the foot to remain on the ground, stretching the back of the foot and the front of the lower leg, which leads to better extension in the ankle joint. If the cramp has already occurred, this alone will probably no longer help; instead, squat briefly, standing only on the balls of your feet and toes and letting your heels sink to the maximum. This is usually enough to continue virasana after half a minute to a minute. Cofactors of the tendency to cramp are cold and frequent or prolonged demands on the feet such as walking, standing, running and, of course, poor footwear. Working on the flexibility of the foot (sole) muscles with a thin fascia roll is then highly recommended.
- The more the buttocks are pulled back, the more you can sit on the center or even the front edge of the ischial tuberosities, which makes it much easier to sit up straight and tires the back muscles less quickly. Flexible short hip extensors are a prerequisite.
- Virasana is one of the difficult poses for the knee joint, which in turn is one of the most sensitive joints in the human body. Therefore, don’t force anything, but approach knee-related poses a little more defensively and differentiate precisely between physiological pain sensations, such as those that occur when muscles are stretched intensively, and non-physiological pain in joints.
- It is quite normal for untrained people to be able to stretch their knee joints again after 5-10 minutes of virasana only after about 1-3 minutes. However, immediately stretching the knee joint after virasana while overcoming the pain that occurs has no negative effect as far as is known. With increasing practice, the knee joints can be stretched again noticeably faster, later without any delay. As in supta virasana, to gradually learn to stretch the knee again, we recommend the dog pose head downwards followed by the upface dog as a test under load on the knee-extending muscles(quadriceps). In virasana, the knee joint is flexed with significantly more pressure than in supta virasana; this is subjectively perceived as a clear difficulty when stretching the knee joint after virasana. The reason for this is that in virasana the entire weight of the upper body including the head is transferred almost 100% into the flexion of the knee joint, but not in supta virasana due to the shoulders, back or head being laid down. In comparison, the difficulty in extending the knee joint can be felt even more in supta virasana because the hamstrings with the biarticular parts in a very short sarcomere length close to the active insufficiency is involved in the reduction of flexion in the hip joint, but the monoarticular caput breve of the biceps is in the shortest sarcomere length for minutes and contracts.
- virasana is an intensive stretch for the three monoarticular parts of the quadriceps, but not for the biarticular rectus femoris due to the flexion in the hip joint. Prolonged practice of virasana without supta virasana or other intensive stretches for the rectus femoris can therefore lead to an imbalance in the thigh muscles with unpleasant symptoms in the knee joint. A good recommendation is therefore to always practise supta virasana after virasana and to do so at least as long and intensively, preferably longer. Instead of supta virasana, you can also practise one of the two quadriceps stretches on the wall(1 or 2).
- As with all yoga poses, the following also applies here: if you no longer feel any effect and no new challenge is in sight or possible, the exercise should not (or no longer) be practiced, at most from time to time to test the status
Known problems that can occur even when executed correctly
Knee pain
In principle, known or unknown pathological changes in the knee joint can always cause pain, even when performed correctly. If these persist during posture and can be reproduced again and again, if the pain cannot be relieved with all the tricks known to us, if the knee joints make themselves felt in other postures, in everyday activities or in sport, this is an invitation to have this clarified by a doctor. The diagnosis is usually made on the basis of the symptoms, a medical history (especially the movement history), a physical examination and, if necessary, three-dimensional imaging using MRI. Arthroscopy to make a diagnosis is no longer state of the art and should not be accepted by the patient. Superfluous arthroscopies should be avoided at all costs, not least because they represent a risk of infection for an extremely immunocompromised area of the body. Even the purely diagnostic arthroscopies without intervention that were still permitted in the past often led to a deterioration in the patient’s condition. In addition, many patients report long-term worsening of their condition after initial improvements, for example if part of the meniscus has been removed. The study situation on this is quite clear. Even if an arthroscopy is economically much more profitable than an MRI plus anamnesis, physical examination including tests and consultation, this should not tempt any doctor, whether in private practice or employed in a clinic, to act against the patient’s best interests. Conservative therapy is very often superior in the long term. As a rule, the body’s own structures are optimal and cannot be replaced by any technical product without disadvantages. Furthermore, medicine is progressing and no one should, without necessity, make potentially superior future treatment options such as stem cell therapy for the regeneration of cartilage or menisci inaccessible to them through hasty or ill-considered intervention. In our view, it is better to try to achieve a stable and resilient improvement in the patient’s condition with exercise and sports therapy, yoga, physiotherapy, osteopathy and other procedures. Even if this means considerably more work and effort of various kinds, it is much more sustainable in the long term and the prognosis of surgical intervention without conservative accompanying procedures, especially movement training and movement therapy, is all too limited.
Variants
Forward bend (balasana)

Instructions
- Do virasana as described above.
- Bend forward from the hips and rest the upper body on the thighs and, if possible, the head on the floor. If the forehead does not reach the floor, it can be placed on a block if it is otherwise too uncomfortable.
- There are two variations of this forward bend:
- with the arms placed forward in an overhead position, which are passively laid down after being stretched once.
- with the arms placed backwards next to the upper body and legs.
Details
- This pose, also known as child’s pose or balasana, is a largely passive pose that has an introverting and calming effect due to its forward-bending construction; this is all the more true when the head is lowered.
- The pelvis and buttocks continue to sink towards the floor, as in virasana. However, there is considerably less gravity available to push the buttocks towards the floor. In cases of less mobile quadriceps, the buttocks will therefore not reach the floor and there may even be a gap between the height of the heels and the buttocks, which can cause a certain amount of tilting forward and reduce the relaxing effect somewhat.
- As in virasana, if the pose is not built up from a properly constructed virasana, the calves should be turned out and the knees pulled forward.
- Rarely, a spasm can occur in the rectus femoris, which should subside when the body pulls forwards and downwards with less load and thus the hip joints are pulled less from the upper body into flexion. In these cases, the head and arms should be placed on appropriate support.
- In some cases, there is a clear stretch in the autochthonous back muscles, which is a sign that they are in urgent need of relaxation and stretching.
- If discomfort occurs in the neck, the flexion of the cervical spine must be changed accordingly so that this discomfort disappears. If there are disc problems in the cervical spine, it must of course be flexion-free.
- This pose is ideal for relaxing the neck muscles after the headstand following their prolonged work. As a rule, if the neck muscles feel tense after leaving the headstand, this discomfort will increase at the beginning in this forward bend, but will almost always disappear more quickly than without it. Variation 2 is particularly suitable for this purpose.
- In cases of significant discomfort in one or both knee joints, the buttocks can be placed on a support so high that the discomfort no longer occurs.
- In addition to the possibly limited sinking of the pelvis to the floor, forward flexion from the hip joints can also be restricted; the extensors of the hip joint (e.g. the gluteus maximus) or, in rare cases, even the hamstrings are responsible for this.
- In the forward bend, the vertebrae should emerge recognizably and reasonably evenly. This can be seen through (thinner) clothing and is also easy to palpate with the fingers, both by a supporter and by the performer with one hand. Normally, the protrusion increases from the lumbar spine to the thoracic spine up to a maximum and then slowly decreases again in the direction of C7. If the vertebrae emerge unevenly, e.g. if one remains ventral (shifted towards the sternum ) or dorsal (protruding backwards) or is noticeably rotated in the plane, this indicates an anomaly that may require treatment or at least clarification.
prasarita forward bend

Eased forward bend
Instructions
- From virasana, open the knees so that the upper body can come to rest between the knees and bend forward.
- If possible, rest your forehead on the floor.
Details
- In addition to the pure facilitation of the forward bend, breathing in the forward bend is also made easier, which is due to the fact that the breathing excursion is less hindered by the pressure of the upper body on the thighs.
- In more advanced pregnancy it is obligatory to perform this variant instead of the normal one.
Supports

Reduction of discomfort in the knee
Instructions
- Take the pose as described above, but place your bottom on a support that is high enough to prevent discomfort in your knees.
Details
- Many abnormal sensations in the knee joint are dependent on load and, in particular, flexion angle. Some of them only occur when the knee is bent far. Many of the abnormal sensations are an expression of unphysiological conditions or events in the knee joint and should be avoided. Roughly speaking, if the sensation is not purely muscular (as far as the performer is able to perceive and assess this), it is generally not tolerable. In some cases, however, knee pain that is only minor AND improves within a reasonable period of time while performing the posture can be tolerated. If knee pain dependent on the flexion of the knee joint (s) occurs, the flexion anglein the knee joint can be reduced by supporting the posture and pain relief can often be achieved. In some (!) of the cases, this pain sensation is dependent on the tension of the monoarticular quadriceps partsand a decrease in the tendency to this pain can be observed with repeated execution. Pain phenomena that cannot be clearly identified as muscular also include stretching sensations in the part of the distal quadriceps tendon that merge into the medial and lateral p atellar retinaculum.
Lower leg supported
Instructions
- take the pose as described above, but do not rest your lower legs on the floor but on shoulder resting plates so that your feet are unsupported.
Details
- This variant makes the posture feasible if there are injuries to the feet or ankle joints that make the standard variant impossible to perform. These can be injuries or diseases of the lower or upper ankle joints or other joints in the foot, a fracture of a tarsal bone, significant shortening of the foot lifts or painful misalignments of tarsal bones.
- The support of the lower leg creates a distance between the tibia and the ground, which on the one hand relieves the ankle joint so that it only has to plantarflex according to gravity, and on the other hand also takes pressure off the bones and structures of the foot and eliminates bending moments in the joints between the bones of the foot.
Mat in the knee

Avoiding knee pain
Instructions
- Do virasana as described above.
- Raise your buttocks again, turn out your calves once more and place a rolled-up mat firmly on your knees from behind.
- Sit between your lower legs again, with the mat limiting the flexion of the knee joint.
Details
- The mat limits the flexion of the knee joint by taking up space between the lower leg and thigh and keeping them apart. This naturally leads to less flexion of the knee joint, but also to increased compression, especially of the calves. If this is felt to be unbearable, the variant with the buttocks on the block proves to be the more practical way of relieving the knee joint.
Known problems that can occur even when executed correctly
Massive pressure sensation in the calf
Compression of the muscles can lead to subjectively unpleasant pressure.