yogabook / joints / scapulothoracic sliding bearing
Contents
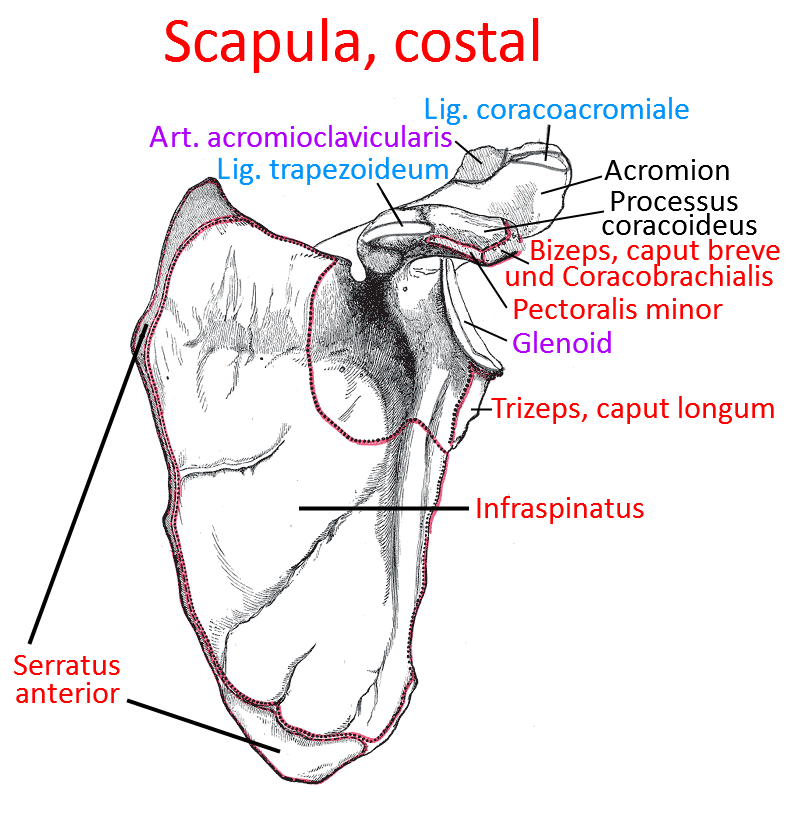
Image: Scapula from costal/ventral (Linkmap)
Scapulothoracic plain bearing
From an anatomical point of view, the scapulothoracic joint is not a true joint because it lacks features of a true joint such as articular cartilage; it is therefore regarded as a secondary joint of the glenohumoral joint and is often referred to as the scapulothoracic glenoid joint. The scapulothoracic joint is the sliding connection of the scapula on the dorsal thorax. The scapula is only guided and held in place by all the muscles listed above. Consequently, this also means that these muscles also hold the arm and any weight hanging from it throughout the day, which explains the tendency to fatigue and tension, particularly in elevators such as the levator scapulae and the trapezius. Posture plays a significant role here, for example a habitually slightly raised shoulder blade is very likely to cause these two muscles to become tense. Between full protraction and retraction, there is a state of maximum lateralization of the scapula, i.e. it is already at almost maximum lateral distance from the spine without any discernible ventral movement having taken place. This position of lateralization is important for many asanas, such as trikonasana or 2nd warrior pose. External rotation of the shoulder blade is a prerequisite for raising the arm beyond about 90°, as otherwise the humerus would touch the acromion. Movements in the scapulothoracic joint are always accompanied by movements in the sternoclavicular and acromioclavicular joints. Of the following depressors, the latissimus dorsi acts directly and indirectly (via the glenohumeral joint because it attaches to the upper arm) on the scapula, the pectoralis major only indirectly. The pectoralis major protractor acts indirectly (via the glenohumeral joint because it attaches to the upper arm) on the shoulder blade because it attaches to the upper arm, while the others act directly. The latissimus dorsi retractor acts directly and indirectly on the shoulder blade, while the other muscles act directly. All external rotators act directly on the shoulder blade. Internal rotation: the latissimus dorsi acts directly and indirectly on the shoulder blade, the rhomboideus major only indirectly, all other external rot ators act directly on the shoulder blade.
Articulating bones
Movement
The shoulder blade can move three-dimensionally on the thorax:
Depression/elevation, protraction/retraction, external rotation, internal rotation. The movements in detail with executing muscles:
Depression: direct: trapezius, serratus anterior; indirect: latissimus dorsi, pectoralis minor, pectoralis major
Elevation (all the elevators mentioned act directly on the shoulder blade): Trapezius, levator scapulae, rhomboideus major, rhomboideus minor, serratus anterior,
Protraction: serratus anterior, pectoralis minor, pectoralis major
Retraction: trapezius, rhomboideus major, rhomboideus minor, latissimus dorsi
External rotation: trapezius, serratus anterior
Internal rotation: latissimus dorsi, levator scapulae, pectoralis minor, pectoralis major, rhomboideus major, rhomboideus minor
Pathology
Some disorders of the joint: Tension of the levator scapulae and trapezius, for example due to constantly slightly elevated shoulder blades, is relatively common. Other habitual factors such as a kyphosis of the thoracic spine plus a recognizably protracted scapula are also quite common. Innervation disorders of the protractors or retractors can cause images such as the scapula alata. Scapular dyskinesia is also possible.
Tests
Tests of the scapulothoracic „joint“
Tests of the movement directions
Tests of the spanning muscles
Latissimus dorsi
Images
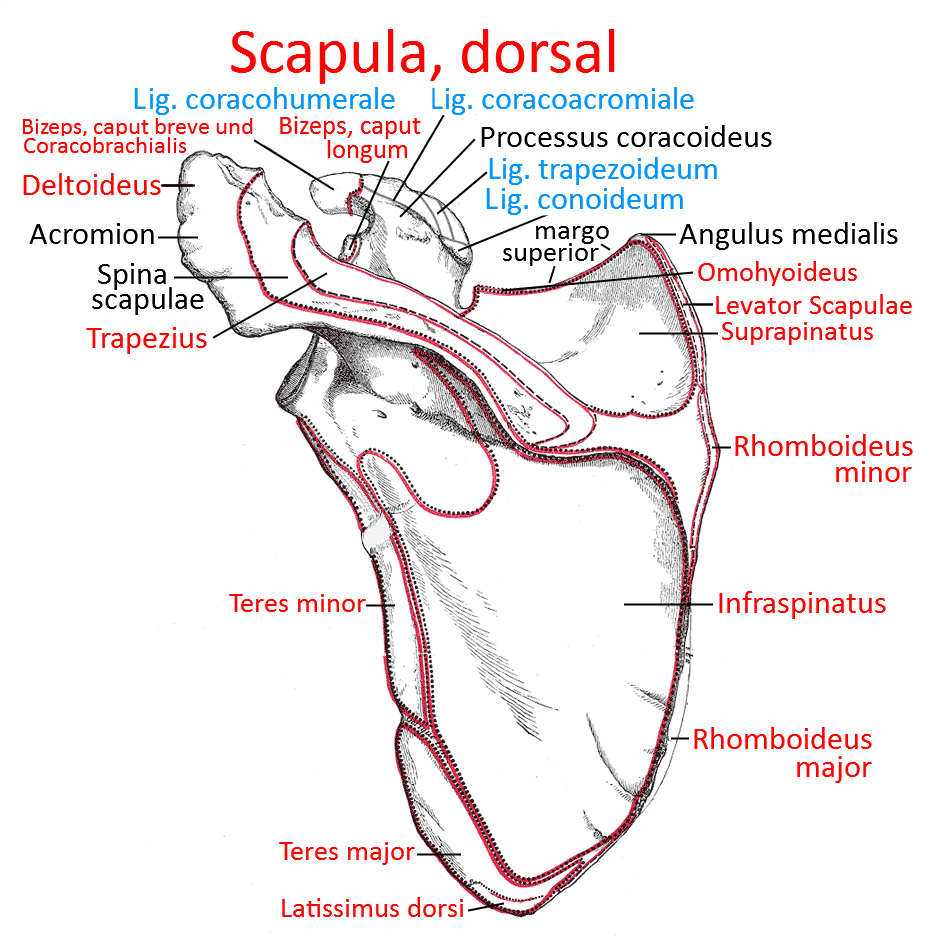
Scapula from dorsal