yogabook / joints / shoulder joint
Contents
- 1 Image: Shoulder joint (Linkmap)
- 2 Articulating bones
- 3 Shoulder joint (glenohumeral joint)
- 4 The movements and the muscles involved
- 5 Ligaments
- 5.1 Acromioclavicular ligament
- 5.2 Inferior acromioclavicular ligament
- 5.3 Lig. acromioclaviculare superius
- 5.4 Lig. conoideum
- 5.5 Coracoacromial ligament
- 5.6 Coracoclavicular ligament
- 5.7 Coracoglenoid ligament
- 5.8 Coracohumeral ligament
- 5.9 Ligg. glenohumeralia
- 5.10 Inferior glenohumeral ligament
- 5.11 Medial glenohumeral ligament
- 5.12 Lig. glenohumerale superius
- 5.13 Lig. transversum humeri
- 5.14 Lig. transversum scapulae inferius
- 5.15 Lig. transversum scapulae superius
- 5.16 Lig. trapezoideum
- 6 Schleimbeutel (Bursae)
- 6.1 Bursa costoclavicularis
- 6.2 Bursa infracoracoidea
- 6.3 Bursa Lig. coracoclavicularis
- 6.4 Bursa pectoralis majoris
- 6.5 Bursa pectoralis minoris
- 6.6 Bursa serratus anterior superior
- 6.7 Bursa serratus anterior inferior
- 6.8 Subacromial bursa
- 6.9 Bursa subcoracoidea
- 6.10 Bursa subcutanea acromialis
- 6.11 Bursa subdeltoidea
- 6.12 Bursa subtendinea infraspinati
- 6.13 Bursa subtendinea latissimus dorsi
- 6.14 Bursa subtendinea subscapularis (subscapular recess)
- 6.15 Bursa subtendinea teretis majoris
- 6.16 Bursa trapezoidea
- 7 Pathology
- 8 Tests
- 9 Pictures
- 9.1 Shoulder joint, capsule and ligaments (image links to linkmap)
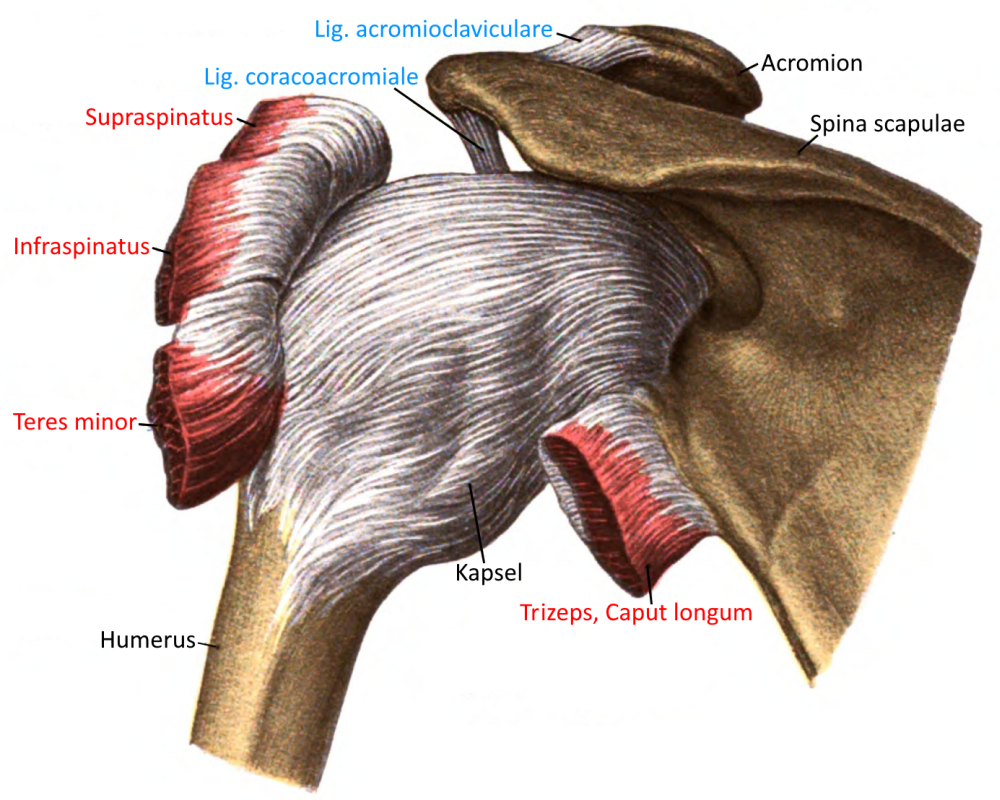
- 9.2 Shoulder joint from dorsal (image links to linkmap)
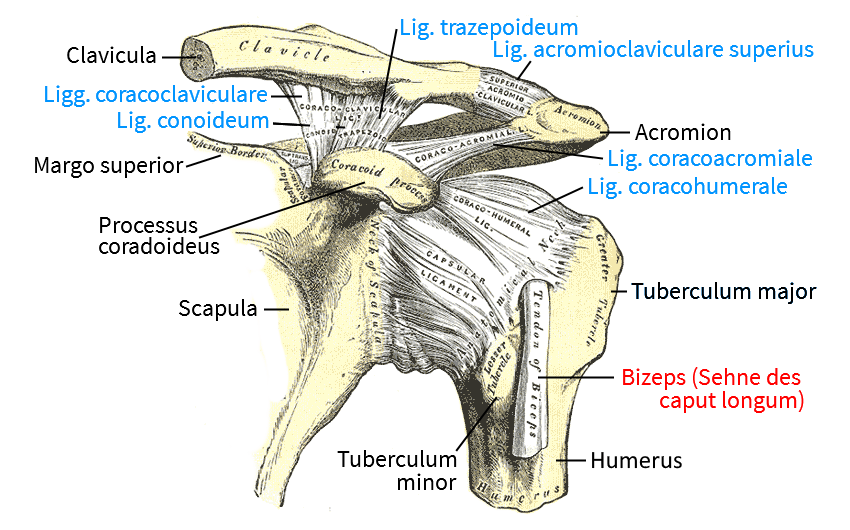
- 9.3 Shoulder joint, ligaments
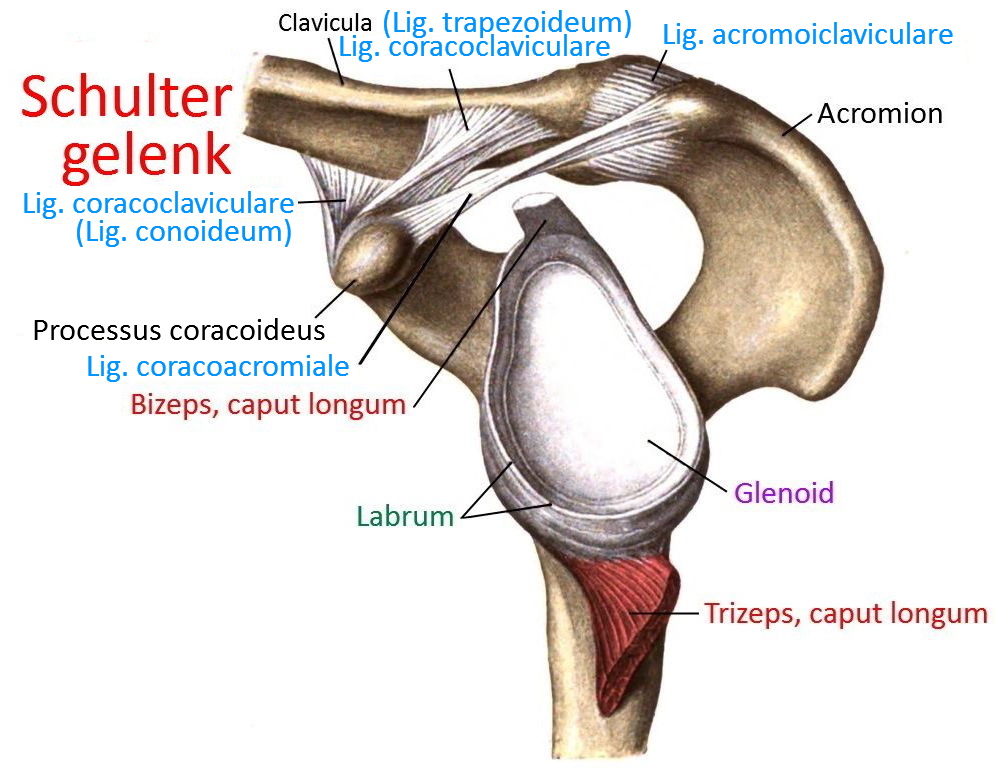
- 9.4 Glenoid (image links to linkmap)
- 9.5 Ligaments (image links to linkmap)
- 9.6 Ligaments (image links to linkmap)
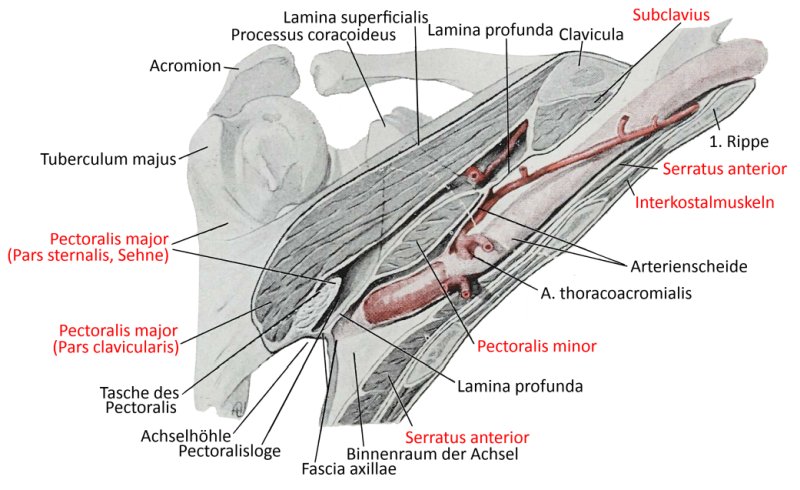
- 9.7 Shoulder joint from ventral (image links to linkmap)
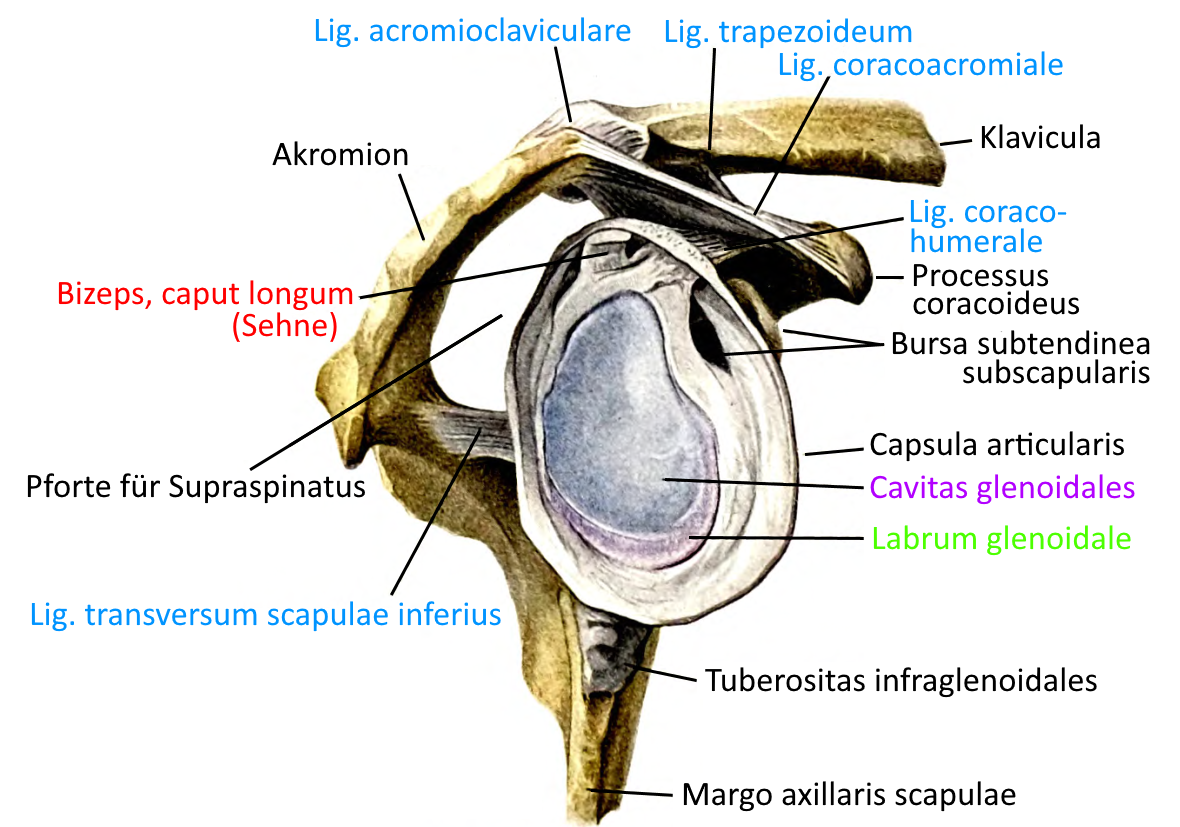
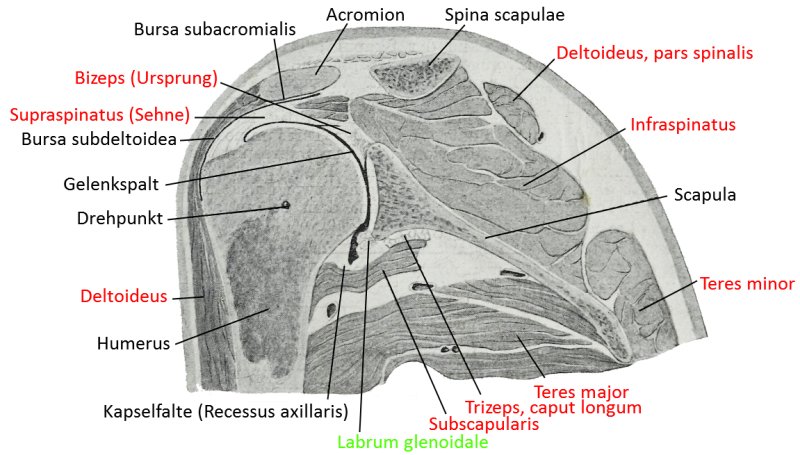
- 9.8 frontal section (image links to linkmap)
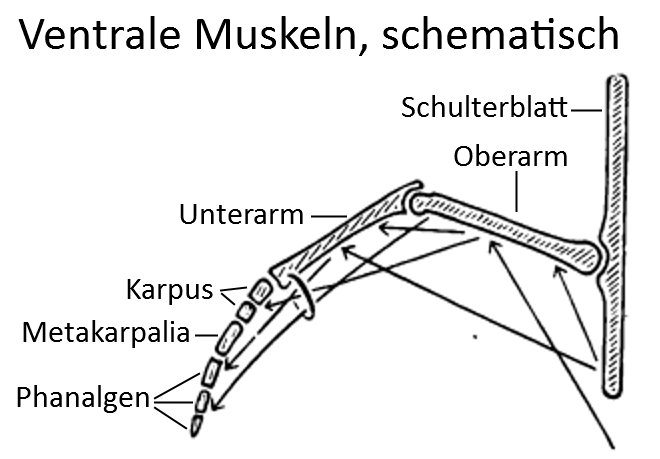
- 9.9 Ventral muscles: scapula to fingers
Image: Shoulder joint (Linkmap)
Ligaments of the shoulder joint see unten.
Articulating bones
Shoulder joint (glenohumeral joint)
The shoulder joint is the joint in which the upper extremity arm can be moved relative to the upper body (more precisely: to the shoulder blade). According to the literature, the shoulder joint is defined as the glenohumeral joint (the shoulder blade-arm joint in which the head of the humerus lies medial to the scapula, the joint surface is called the glenoid) and the non-acromiohumeral joint (the shoulder blade-arm joint in which the head of the humerus lies dorsal-cranially at a certain distance (0.8 – 1 cm) below the acromion (shoulder height) ). However, these do not provide the full range of movement that we know from the arm; it is only made possible together with the movement of the shoulder blade on the back: it can be rotated outwards in its plane below(external rotation) and moved forwards(protraction) and backwards(retraction) as well as upwards(elevation) and downwards(depression).
The shoulder-arm joint already enables three-dimensional movement: lateral(lateral abduction), frontal(frontal abduction, also known as anteversion) and rotation(endorotation / exorotation) of the arm. In addition to the glenohumeral and acromiohumeral joint, the „shoulder joint“ also includes the acromioclavicular joint, in which the scapula is supported by the movable collarbone(clavicle) (on the other side, the clavicle lies against the sternum in the sternoclavicular joint ) and the scapulothoracic „joint“ (more precisely: scapulothoracic gliding bearing), in which the scapula is separated from the thorax by two muscles(serratus anterior and subscapularis) i.w. freely movable on the back.
The movements and the muscles involved
lateral abduction: M. deltoideus, M. supraspinatus, M. biceps brachii (caput longum), subscapularis (cranial fibres)
lateral adduction: triceps (caput longum), M. teres major, M. teres minor, latissimus dorsi, pectoralis, M. deltoideus (partly together with pars spinalis und pars clavicularis)
frontal abduction (anteversion): M. deltoideus (pars clavicularis), Bizeps, M. pectoralis major (pars clavicularis, pars sternocostalis), M. coracobrachialis
frontal adduction / retroversion: M. teres major, M. latissimus dorsi, triceps (caput longum), M. deltoideus (pars spinalis, pars acromialis partly)
Exorotation: M. infraspinatus (strongest), M. teres minor, M. deltoideus (pars spinalis)
Endorotation: M. subscapularis (kräftigster), M. pectoralis major, M. biceps brachii (caput longum), M. deltoideus (pars clavicularis), M. teres major, M. latissimus dorsi
Ligaments
The shoulder joint has only a few ligaments, which do not provide sufficient guidance in view of the large traffic area of the joint:
- Acromioclavicular ligament (ACG)
- Lig. acromioclaviculare inferius
- Lig. acromioclaviculare superius
- Lig. conoideum (Teil des Lig. coracoclaviculare)
- Lig. coracoacromiale (ACG)
- Lig. coracoclaviculare(Lig. trapezoideum und Lig. conoideum)
- Lig. coracoglenoidale
- Lig. coracohumerale
- Ligg. glenohumeralia
- Lig. glenohumerale inferius
- Lig. glenohumerale mediale
- Lig. glenohumerale superius
- Lig. transversum scapulae inferius
- Lig. transversum scapulae superius
- Lig. transversum humeri
- Lig. trapezoideum (part of the coracoclavicular ligament) (ACG)
This only comes from the muscles covering the shoulder joint, especially the so-called rotator cuff. The transverse humeral ligament is not strictly speaking part of the shoulder joint; it holds the tendon of origin of the long head of the biceps in the intertubercular sulcus. The ligaments of the shoulder joint are as follows:
Acromioclavicular ligament
The acromiclavicular ligament connects the acromion to the scapula. Two fiber courses can be distinguished.
Images:
Linkmap: Acromioclavicular joint
Linkmap: Glenoid
Linkmap: Ligaments of the shoulder joint
Inferior acromioclavicular ligament
strengthens the caudal area of the joint capsule and is connected to the supraspinatus.
Pictures: (still without)
Lig. acromioclaviculare superius
reinforces the superior joint capsule of the acromioclavicular joint as a quadrangular ligament. It runs from the cranial distal clavicle to the neighboring acromion. Its fibers radiate into the fascia of the trapezius and deltoid. The cranial superior acromioclavicular ligament is stronger than the caudal inferior acromioclavicular ligament.
Images:
Linkmap: Ligaments of the shoulder joint
Lig. conoideum
The conoid ligament is the part of the coracoclavicular ligament that attaches to the conoid tubercle of the clavicle.
Images:
Linkmap: Ligaments of the shoulder joint
Linkmap: Ligaments of the shoulder joint
Linkmap: Glenoid and ligaments
Linkmap: Acromioclavicular joint
Linkmap: Scapula from dorsal, insertions
Linkmap: Clavicle with insertions
Coracoacromial ligament
The coracoaromial ligament is a strong band that connects the coracoid process to the underside of the acromion in a triangular shape. The pointed end attaches directly in front of the acromioclacivular joint. The broad side covers the entire length of the coracoid process. Cranially it lies below the deltoid and caudally it is connected to the supraspinatus by a bursa. The coracoaromial ligament forms the „acromion“ together with the acromion and the coracoid process.
Images:
Linkmap: Acromioclavicular joint
Linkmap: Glenoid and ligaments
Linkmap: Glenoid and surroundings
Linkmap: Shoulder joint, ligaments
Linkmap: Shoulder joint, ligaments
Linkmap: Scapula from dorsal, insertions
Linkmap: Scapula from costal view, insertions
Coracoclavicular ligament
The coracoclavicular ligament is a two-part ligament that attaches the underside of the clavicle to the coradoid process of the scapula: Lig. trapezoideum and Lig. conoideum.
Images:
Linkmap: Acromioclavicular joint
Linkmap: Ligaments of the shoulder joint
Linkmap: Ligaments of the shoulder joint
Coracoglenoid ligament
The coracoglenoid ligament runs from the coracoid process to the joint capsule and the glenoidlabrum, on the upper side of which it attaches.
Images: (no picture yet)
Coracohumeral ligament
The coracohumeral ligament connects the coracoid process to the humerus and has an anterior part that runs from the lateral edge of the base of the coracoid process to the lesser tuberosity of the humerus and a posterior part that connects the greater tuberosity to the coracromial ligament. Cranially and ventrally it is overgrown with the joint capsule and lies caudal to the supraspinatus and cranial to the supscapularis. In addition to its general shoulder-stabilizing function, it helps to secure the tendon of the caput longum of the biceps and limits the caudal descent of the humerus. Due to its course, it limits lateral abduction without exorotation.
Images:
Linkmap: Glenoid and surrounding area
Linkmap: Ligaments of the shoulder joint
Linkmap: Ligaments of the shoulder joint
Linkmap: Dorsal view of the scapula: insertions
Ligg. glenohumeralia
The glenohumeral ligaments reinforce the ventral joint capsule as three capsular ligaments. They originate at the supraglenoid tubercle of the scapula from fibers of the glenoidlabrum and run as a capsular ligament to the collum anatomicum of the humerus. They appear as three folds in the joint capsule. These are differentiated from cranial to caudal as:
- Superior glenohumeral ligament (SGHL)
- Medial glenohumeral ligament (MGHL)
- Inferior glenohumeral ligament (IGHL)
Inferior glenohumeral ligament
the strongest of the three ligaments, which has two courses, one anterior and one posterior. Between these, the joint capsule forms the recessus axillaris. It opposes translation caudally, ventrally and dorsally, the more the arm abducts laterally. If the anterior part of this ligament tears together with a tear in the glenoidlabrum, as can happen with shoulder dislocations, this is called a Bankart lesion.
Images: (still without)
Medial glenohumeral ligament
a stronger ligament that varies significantly from person to person. It stabilizes against ventral translation, especially in mid-lateral abduction.
Images: (not yet available)
Lig. glenohumerale superius
The superior glenohumeral ligament is a narrow, thin ligament which, together with the coracohumeral ligament, stabilizes the anatomically null proximal and laterally adducted arm.
Images: (still without)
Lig. transversum humeri
The transverse ligament of the humerus runs over the intertubercular sulcus of the humerus and tensions and holds the tendon of origin of the long head of the biceps in the sulcus. It therefore connects the greater tuberosity of the humerus and the lesser tuberosity of the humerus. Opinions differ as to whether the transverse humeral ligament is a true ligament or rather a fibrous extension of the subscapularis.
Images: (still without)
Lig. transversum scapulae inferius
The inferior transverse scapular ligament is present inconstantly. It runs from the lateral edge of the scapular spine to the dorsal edge of the glenoid.
Images:
Linkmap: Glenoid and surroundings
Lig. transversum scapulae superius
The lig. transversum scapulae superius is an inconstant ligament that runs from the lateral edge of the scapular spine of the scapula to the dorsal edge of the glenoid.
Images:
Linkmap: Shoulder joint, ligaments
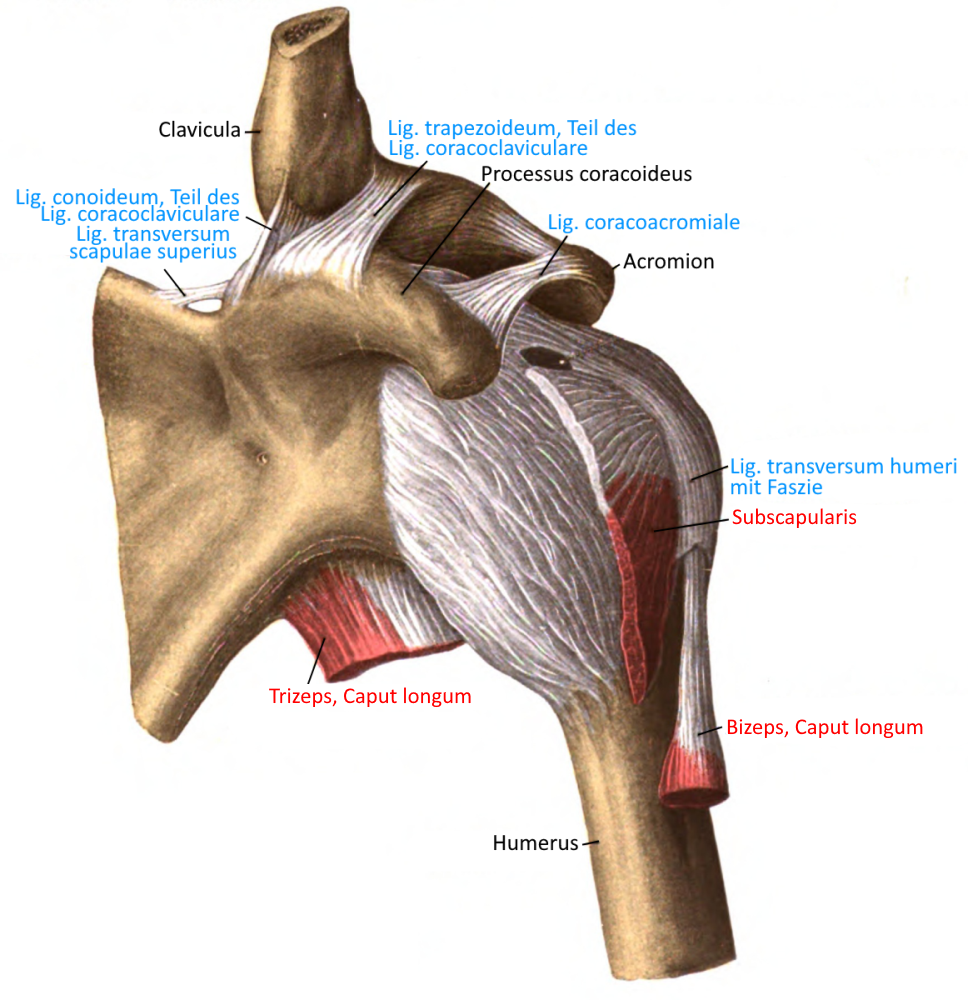
Linkmap: Shoulder joint with scapula, ventral, profound
Linkmap: Shoulder joint with scapula, ventral, superficial
Linkmap: Shoulder joint with scapula, medioventral
Lig. trapezoideum
The trapezoid ligament is the part of the coracoclavicular ligament that attaches to the trapezoid line of the clavicle.
Images:
Linkmap: Shoulder joint, ligaments
Linkmap: Shoulder joint, ligaments
Linkmap: Acromioclavicular joint
Linkmap: Glenoid and ligaments
Linkmap: Glenoid and surroundings
Linkmap: Scapula from dorsal, insertions
Linkmap: Scapula from costal view, insertions
Linkmap: Scapulothoracic gliding bearing
Linkmap: Clavicle with insertions
Schleimbeutel (Bursae)
Bursa costoclavicularis
Bursa located between the two parts of the sternoclavicular ligament(anterior sternoclavicular ligament and posterior sternoclavicular ligament).
Bursa infracoracoidea
Non-communicating bursa between the tip of the coracoid process, extending along the tendon of the short head of the biceps to the joint capsule.
Bursa Lig. coracoclavicularis
Non-communicating bursa located between the conoid ligament and the trapezoid ligament.
Images: (still without)
Bursa pectoralis majoris
Non-communicating bursa between the attachment tendon of the pectoralis major and the tendon of the biceps, caput longum.
Bursa pectoralis minoris
Rare, inconstant, non-communicating bursa between the attachment tendons of the subscapularis and pectoralis major.
Bursa serratus anterior superior
Bursa between subscapularis and serratus anterior to the superior scapular angulus. It can communicate with an inconstant bursa accessoria.
Bursa serratus anterior inferior
Submuscular bursa between the serratus anterior and the chest wall at the angulus inferior scapulae. It can communicate with an inconstant bursa accessoria.
Subacromial bursa
large bursa between the attachment tendon of the supraspinatus and other neighboring structures such as the acromion, coracoid process, coracromial ligament and deltoid. It communicates with the subdeltoidbursa.
Images: (still without)
Bursa subcoracoidea
Bursa between the root of the coracoid process and the subscapularis, which already runs as a tendon. It communicates with the joint cavity and the subtending subscapularisbursa.
Images:
Linkmap: Shoulder joint, ligaments
Bursa subcutanea acromialis
Non-communicating subcutaneous bursa over the acromion.
Images: (still without)
Bursa subdeltoidea
Bursa between the deltoid and the capsule of the shoulder joint. It extends under the acromion and the coracoacromial ligament and communicates with the subacromialbursa.
Images:
Linkmap: Shoulder joint, sectional view
Bursa subtendinea infraspinati
Rarely communicating bursa between the insertion tendon of the infraspinatus and the capsule of the shoulder joint
Images: (still without)
Bursa subtendinea latissimus dorsi
Bursa between the attachment tendon of the latissimus dorsi and that of the teres major.
Bursa subtendinea subscapularis (subscapular recess)
Bursa between the attachment tendon of the subscapularis and the tendon of origin of the coracobrachialis on the one hand and the capsule of the shoulder joint on the other. Ventrally there is an opening to the joint cavity of the shoulder joint (Weitbrecht’s foramen) which breaks through the joint caps ule and glenohumeral ligament. The bursa communicates with the subcoracoidbursa and the joint capsule.
Images:
Linkmap: Glenoid and surroundings
Bursa subtendinea teretis majoris
Non-communicating bursa located between the attachment tendon of the teres major and the ventromedial humerus close to the attachment.
Bursa trapezoidea
Inconstant bursa caudal to the trapezius near its attachment to the scapula and spina scapulae
Pathology
The shoulder joint is dependent on good muscle guidance due to the small surface area and wide opening of the glenoid. It is therefore more susceptible to injury than the hip joint.
- Impingement syndrome
- Frozen shoulder (periarthritis humeroscapularis)
- Tendinosis calcarea (calcified shoulder)
- Osteoarthritis
- Cervical spine syndrome
- Dislocation(dislocation, luxation)
- Ligament stretching
- SLAP lesion
Instabilities of the shoulder joint are not uncommon. In young people between the ages of 10 and 12, they are usually caused by a classic injury sustained during sport and leisure activities. Causes can be external rotation-abduction trauma or direct trauma as well as repeated microtrauma. The Gerber classification is divided into 6 stages:
- hooked dislocation
- unidirectional instability without hyperlaxity
- unidirectional instability with hyperlaxity
- multidirectional instability without hyperlaxity
- multidirectional instability with hyperlaxity
- Arbitrary dislocation
In young people, trauma during overhead sports often plays a role. In 80 to 95% of cases, purely conservative treatment leads to recurrence. In classic external rotation-abduction trauma, the inferior glenohumeral ligament or the medial glenohumeral ligament is often affected.
Degeneration of the rotator cuff begins at the age of 30 and is progressive. The increasing insufficiency is mainly due to reduced perfusion of the tendon tissue close to the insertion. Of the ruptures, 50% are atraumatic. Outlet impingement is frequently associated with a secondary rupture; purely traumatic ruptures are rare and occur in 8% of cases, often in over 40-year-olds with dislocations. Ruptures of the subscapularis are traumatic in 70% of cases and are not recognized in 50% of cases. Ruptures of the supraspinatus tendonor infraspinatus tendondue to previous degenerative damage are common. Above all, overhead athletes often show the combination of subacromial impingement and instability. In the group of shoulder pain in overhead sports
- Primary outlet impingement caused by the subacromial arch
- Primary instability Secondary impingement caused by recurrent microtrauma
- primary instability secondary impingement caused by general hyperlaxity
- Instability caused by macrotrauma without impingement
The indications for surgery include
- Traumatic isolated subscapularis rupture, must be treated within four weeks
- Traumatic rupture in the rotator cuff without previous damage with loss of function
- Rupture in the rotator cuff after shoulder dislocations in working age with assumed good patient compliance
- as a relative indication: acute rupture in the rotator cuff with previous degenerative damage and deep joint-side supraspinatus rupture
Another shoulder lesion with an indication for surgery is Andrews‘ lesion. Repeated traction loads on the long biceps tendonin young overhead throwers lead to detachment of the less vascularized labrum due to the maximum lunging movement. ACG dislocations usually occur when falling on the arm extended forwards and in the case of direct impact trauma, e.g. when falling off a bicycle. The extent of the ligament injury is graded 1 to 3 according to Tossy and generally 1 to 4 according to Rockwood. Typically, Tossy grade 3 or Rockwood grade 3 or 4 lesions are an indication for surgery.
Tests
Tests of the shoulder joint
Instability:
- Load and shift test
- Sulcus sign (lower drawer)
- Shoulder relocation test
- Miniaci Test
- Anterior apprehension test (anterior instability)
SLAP-lesion:
- O’Brien-Sign (Active Compression)
- Biceps load test
- Biceps-Load-2-Test
- Dynamic Labral Shear Test
- SLAP Läsion Test Cluster (SLAP Lesion Cluster)
- Speed-Test
- Yergason-Test
- Active Compression Test
- Passive Distraction Test
Posterior inferior labrum lesion::
Impingement
Mixed:
- Palm up test (Biceps tendinitis, subluxation, subacromial impingement, SLAP-lesion)
Thoracic outlet-Syndrom:
- Roos Test
- Adson Test
- Wright (Hyperabduction-) Test
- Eden-Test (military brace test für den kostal-claviculären Bereich)
GIRD:
General:
Tests of the movement directions
Mobility in general:
Rotation in general:
Internal rotation:
- definite yoga Schulterendorotationstest mit statischer Hand
- definite yoga Schulterendorotationstest in maricyasana
External rotation:
- definite yoga Schulterexorotationstest im Sitzen mit halber Frontalabduktion,
- definite yoga Schulterexorotationstest im Liegen ohne Abduktion
Frontal abduction:
- definite yoga Oberarm-Wand-Test, definite yoga gehaltener Überzug-Test
- definite yoga Schulterfrontalabduktionstest mit erhöhter Rückenausstreckung
Retroversion:
- definite yoga Schulterretroversionstest in uttanasana
- definite yoga Schulterretroversionstest in purvottanasana
Mixed
- Pectoralis-contracture test (Pectoralis major and minor)
Scapulothoracal gliding bearing (scapulothoracic „joint“):
Tests of the spanning muscles
Triceps
Latissimus dorsi
- definite yoga Latissimusflexibilitätstest Schulteröffnung am Stuhl
- definite yoga Latissimusflexibilitätstest im Hundeellbogenstand
Trapezius
Mixed tests
- Scapular-assistance-test (weakness of serratus anterior or trapezius)
- Hornblower-sign (Schwäche der Exorotatoren Teres minor, Infraspinatus)
- Belly-Press-Test (internal rotators)
Supraspinatus
Infraspinatus
Subscapularis
Serratus anterior
Rhomboids
Pictures
Shoulder joint, capsule and ligaments (image links to linkmap)
Shoulder joint from dorsal (image links to linkmap)
Shoulder joint, ligaments
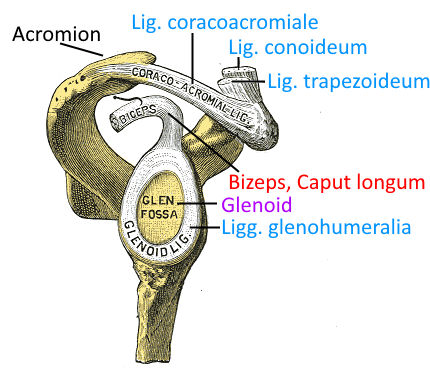
Glenoid (image links to linkmap)
Ligaments (image links to linkmap)
Ligaments (image links to linkmap)
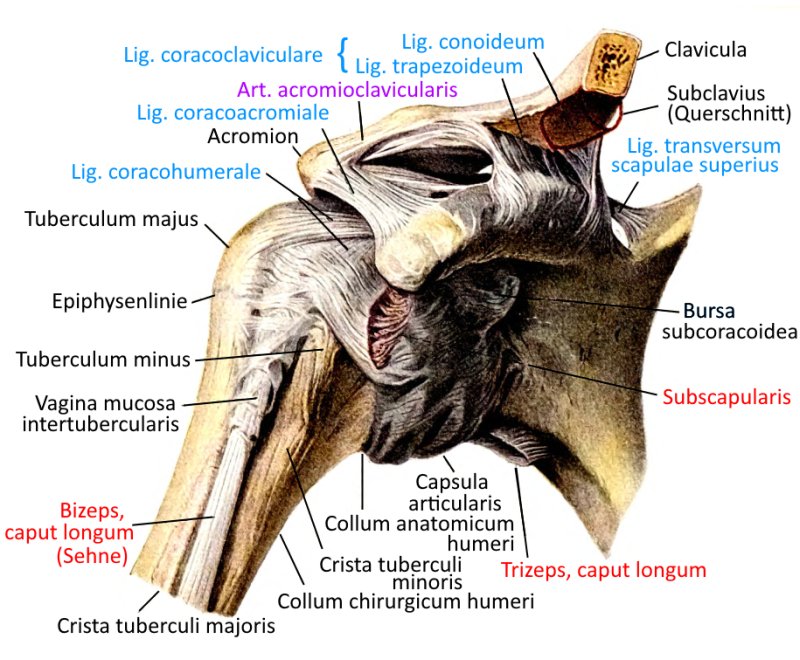
Shoulder joint from ventral (image links to linkmap)
frontal section (image links to linkmap)
Ventral muscles: scapula to fingers